Type 1 diabetes in children: insulin regimens, HbA1c targets and sick day rules
Managing Type 1 Diabetes (T1DM) in children is a classic UKMLA topic, especially focusing on the NICE guidelines. It's all about balancing tight glycemic control with the practicalities of a child's lifestyle.
Insulin Regimens
In the UK, the goal is to mimic physiological insulin secretion as closely as possible. NICE recommends:
- Multiple Daily Injections (MDI): This is the "basal-bolus" approach. It involves a long-acting basal insulin (like Glargine or Detemir) once or twice daily, plus rapid-acting bolus insulin (like Aspart or Lispro) before meals.
- Continuous Subcutaneous Insulin Infusion (CSII/Pump): This is often preferred for younger children or those with frequent hypoglycemia. It provides a continuous basal rate with user-triggered boluses for meals.
HbA1c Targets
For children and young people with T1DM, the NICE target is an HbA1c of 48 mmol/mol (6.5%) or lower. The aim is to achieve this without frequent or "hypos," which can be a tricky balancing act!
Sick Day Rules
When a child with T1DM is ill (even if they aren't eating), their blood glucose usually rises due to stress hormones. The "Golden Rule" is: Never stop insulin.
Key steps include:
- Monitor Frequently: Check blood glucose and ketones every 1–2 hours.
- Hydration: Encourage sugar-free fluids to prevent dehydration.
- Insulin Adjustment: Increase the dose if blood glucose or ketones are rising (often using a "sliding scale" or percentage increase).
- Ketone Management: If ketones are > 0.6 mmol/L, it's a red flag. If they are > 3.0 mmol/L, it's a medical emergency (potential DKA).
I'll find a clear management algorithm for these sick day rules to help you visualize the steps.
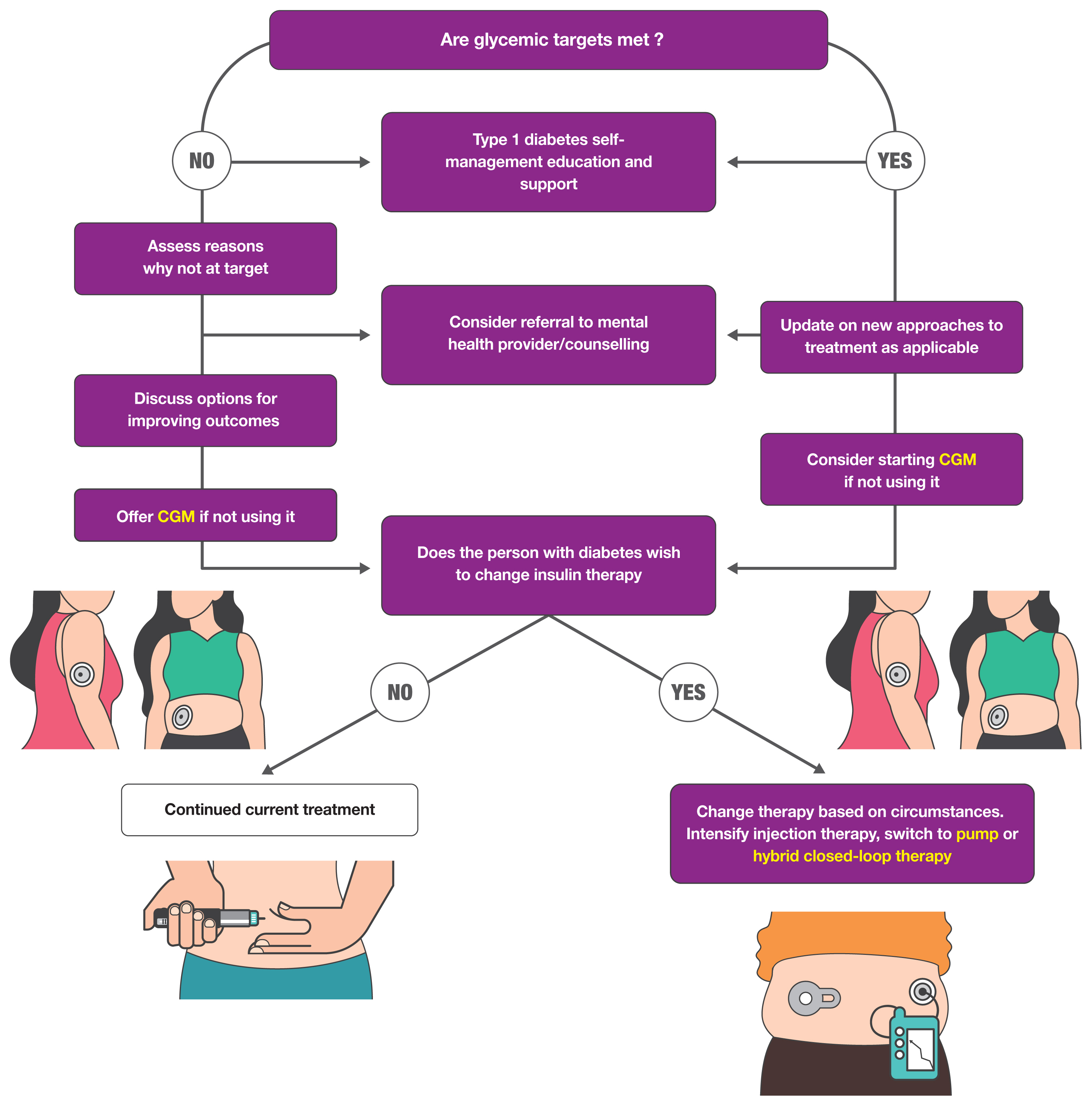
This diagram illustrates the common pathways for managing insulin therapy in children and young people, including the transition between multiple daily injections and insulin pump therapy.
Since sick day rules are so high-yield for the AKT, I've put together a summary table of the key monitoring and action steps based on ketone levels.
| Ketone Level (mmol/L) | Interpretation | Action |
|---|---|---|
| < 0.6 | Normal | Continue usual insulin; check glucose/ketones every 2-4 hours. |
| 0.6 - 1.5 | Slightly elevated | Give extra rapid-acting insulin (usually 10% of total daily dose); recheck in 1-2 hours. |
| 1.5 - 3.0 | High risk of DKA | Give extra rapid-acting insulin (usually 20% of total daily dose); check for vomiting; contact diabetes team. |
| > 3.0 | Emergency | High risk of DKA; seek immediate medical attention/A&E. |
Remember: Always encourage sugar-free fluids to prevent dehydration, but if blood glucose is low (< 11 mmol/L), switch to sugar-containing fluids to allow for continued insulin administration.
This table is a great one to keep in mind for the AKT, as they often ask for the next step in management when a child presents with a high ketone level.
Let me pull up some relevant lessons and flashcards to help you lock this in.
📚 Pediatric T1DM Lessons
Those lessons cover the core management and the emergency side of things like DKA. To help you memorize the specific targets and rules, here are some flashcards.
🗂️ T1DM Flashcards
Tap to study flashcards in the Oncourse app
It looks like those specific queries were a bit too narrow for the flashcards. Let me try a broader search to find some good review cards for you.
🗂️ Diabetes Review Cards
Tap to study 26 flashcards in the Oncourse app
Those cards should help reinforce the basics of insulin and DKA. To wrap things up, here's a quick high-yield summary for your UKMLA prep:
- HbA1c Target: ≤ 48 mmol/mol (6.5%).
- Insulin: Basal-bolus (MDI) is the standard; pumps (CSII) are an alternative.
- Sick Day Rules: Never stop insulin! Check glucose/ketones every 1-2 hours.
- Ketones: > 3.0 mmol/L is an emergency.
Would you like to test your knowledge with a quick game? I can set up a Synapses game to help you categorize different aspects of diabetes management!
Setting up chat...