Tuberculosis: diagnosis, NICE screening and standard treatment regimen
Tuberculosis (TB) is a classic exam favorite, especially for the UKMLA AKT, because the management and screening protocols are so specific. It’s essentially the "great mimicker," so having a solid grasp of the diagnostic pathway is key!
1. Diagnosis of Active TB
When a patient presents with that classic triad of chronic cough, night sweats, and weight loss, here is how we track it down:
- Initial Imaging: A Chest X-ray is the first-line investigation. You're looking for upper lobe infiltrates, cavitation, or hilar lymphadenopathy.
- Gold Standard: Sputum Culture (Lowenstein-Jensen medium). It takes weeks, but it's the definitive way to confirm the diagnosis and check for drug sensitivities.
- Rapid Testing: Nucleic Acid Amplification Tests (NAAT) (like GeneXpert) are used to get a quick diagnosis and check for Rifampicin resistance.
- Microscopy: Acid-fast bacilli (AFB) staining (Ziehl-Neelsen or Auramine-Rhodamine) on three spontaneous sputum samples (including one early morning sample).
2. NICE Screening (Latent TB)
NICE guidelines focus on identifying people at high risk of having "sleeping" TB so we can prevent it from waking up.
- Mantoux Test: This is the traditional skin test. A positive result (induration) suggests prior exposure.
- Interferon-Gamma Release Assay (IGRA): This is a blood test used if the Mantoux is positive or if the patient has had the BCG vaccine (which can cause a false positive Mantoux).
- Who do we screen?
- Close contacts of patients with active pulmonary/laryngeal TB.
- New entrants to the UK from high-incidence countries.
- Immunocompromised patients (e.g., those starting biologics or HIV positive).
3. Standard Treatment Regimen
For active, non-resistant TB, we use the standard "RIPE" acronym. It’s split into two phases:
- Initial Phase (2 months): Four drugs to hit the bacteria hard.
- Rifampicin
- Isoniazid (given with Pyridoxine/Vitamin B6 to prevent peripheral neuropathy)
- Pyrazinamide
- Ethambutol
- Continuation Phase (4 months): Two drugs to finish the job.
- Rifampicin
- Isoniazid
I've put together a quick summary table of the side effects, as these are very high-yield for the AKT.
| Drug | Key Side Effects | Monitoring / Notes |
|---|---|---|
| Rifampicin | Orange secretions (tears/urine), Hepatitis | Potent CYP450 inducer (watch for drug interactions!) |
| Isoniazid | Peripheral neuropathy, Hepatitis | Always co-prescribe Pyridoxine (B6) |
| Pyrazinamide | Hyperuricaemia (can trigger Gout), Hepatitis | Most hepatotoxic of the bunch |
| Ethambutol | Optic neuritis (blurred vision, red-green color blindness) | Check visual acuity before and during treatment |
That table covers the "must-know" side effects that usually pop up in clinical vignettes.
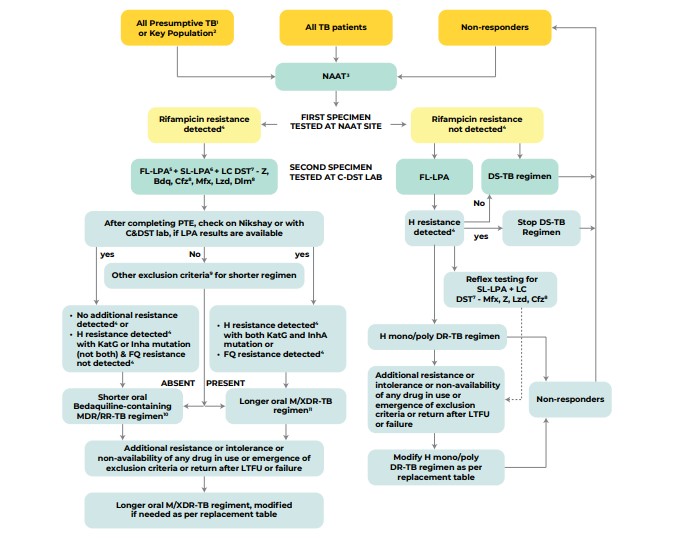
To help you visualize the diagnostic pathway for active TB, let me pull up a clinical flowchart for you.
Here is a flowchart that breaks down the diagnostic pathway, including how we handle drug resistance:
One final high-yield tip for the AKT: Notification. TB is a notifiable disease in the UK. If you suspect it, you must notify the proper authorities (Public Health England/UKHSA) even before the culture results come back!
Would you like to try a few practice questions on this to see how it's tested, or should we look at some flashcards for the drug side effects?
Setting up chat...