Thyroid surgery: indications, complications and post-op management
Thyroid surgery is a classic surgical topic that pops up frequently in the UKMLA AKT, especially regarding the "don't miss" complications. Whether it's a total thyroidectomy for cancer or a hemithyroidectomy for a suspicious nodule, the principles remain the same.
Indications for Thyroid Surgery
We generally take the thyroid out for one of three reasons:
- Malignancy: Confirmed or highly suspicious nodules (e.g., Thy4 or Thy5 on FNA).
- Compressive Symptoms: A large goitre causing "the big three": dysphagia (difficulty swallowing), dyspnoea (difficulty breathing), or stridor.
- Hyperthyroidism: Usually Graves' disease where medical management (carbimazole) has failed, is contraindicated, or the patient prefers a definitive fix.
To help you visualize the delicate structures we're trying to avoid during surgery, let me pull up a diagram of the thyroid anatomy.
As you can see in the diagram, the Recurrent Laryngeal Nerve (RLN) and the Parathyroid Glands are the "VIPs" of the neck—any damage to them leads to the most common post-op issues.
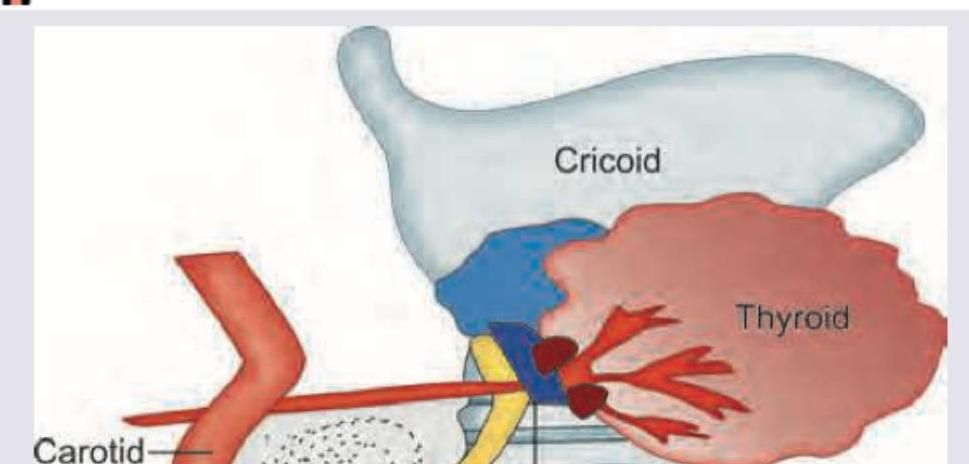
This diagram highlights the close relationship between the thyroid gland, the yellow recurrent laryngeal nerve, and the four small parathyroid glands on the posterior surface.
Complications of Thyroid Surgery
Complications are often categorized by when they occur. The "scariest" one is a tension haematoma, which can cause rapid airway obstruction. If a patient develops a "tight neck" and respiratory distress post-op, the immediate management is to remove the skin clips/sutures at the bedside to release the pressure.
Let me break these down into a clear table for your revision.
| Timing | Complication | Key Features |
|---|---|---|
| Immediate | Haemorrhage / Haematoma | "Tight neck", respiratory distress, stridor. Surgical emergency! |
| Early | Recurrent Laryngeal Nerve (RLN) Injury | Unilateral: Hoarseness. Bilateral: Stridor/Airway obstruction. |
| Early | Hypocalcaemia | Due to parathyroid trauma/removal. Perioral tingling, carpopedal spasm (Trousseau's sign). |
| Early | Infection | Rare in the neck but can occur. |
| Late | Hypothyroidism | Expected after total thyroidectomy; requires lifelong Levothyroxine. |
| Late | Scarring | Hypertrophic or keloid scars can occur in the "necklace" incision. |
Post-Operative Management
The post-op period is all about monitoring for those complications we just talked about. Here's what you'll see on the ward:
- Airway Monitoring: Keep a stitch cutter or clip remover at the bedside at all times. If the patient has a haematoma, you don't wait for the theatre—you open the wound right there to save their life.
- Calcium Levels: We check serum calcium at 6 hours and 24 hours post-op. If the parathyroids were bruised or removed, the calcium will drop. If it's low, we start oral calcium and Vitamin D (Alfacalcidol).
- Thyroid Function: If the whole gland was removed, the patient starts Levothyroxine (usually 100-150mcg) the next morning. We'll check their TFTs in 6 weeks to adjust the dose.
- Voice Check: We always ask the patient to speak as soon as they're awake to check for hoarseness (RLN injury).
I'll pull up some lessons and flashcards to help you lock this in for your AKT!
📚 Thyroid Surgery Lessons
Those lessons cover everything from the surgical technique to the long-term management of thyroid cancer. To make sure you've got those complications and indications memorised, let's pull up some flashcards.
🗂️ Thyroid Surgery Flashcards
Tap to study 6 flashcards in the Oncourse app
Those flashcards are great for testing your knowledge on the nerve anatomy and the specific risks involved.
If you remember only one thing for your exams, let it be the management of post-op respiratory distress: if the neck is swollen and the patient is struggling to breathe, the answer is always to open the wound at the bedside before doing anything else.
Let me know if you want to dive deeper into any of these complications or if you'd like to try a quick quiz on this!
Setting up chat...