Endocrinology: thyroid disorders — hypo vs hyperthyroidism, Graves, Hashimoto
Ah, the thyroid—that tiny butterfly-shaped gland in your neck that basically runs the metabolic thermostat for your entire body! It's a huge topic for the USMLE, especially when you start comparing the "revved up" state of hyperthyroidism versus the "slowed down" state of hypothyroidism.
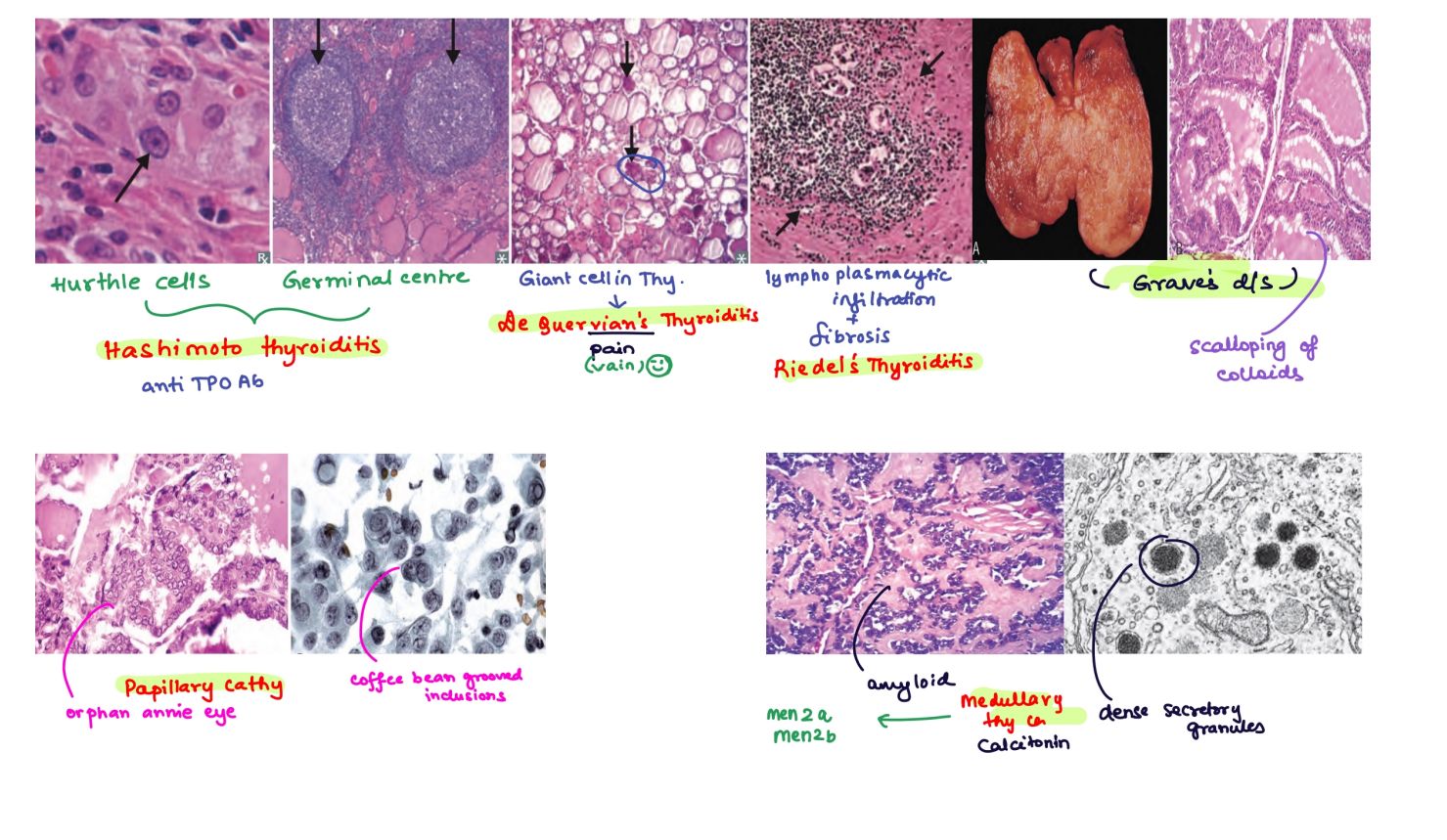
Let me grab a quick visual of the thyroid anatomy and some common pathologies to get us started.
That image gives a great overview of the histopathology you'll need to recognize, like those Hürthle cells in Hashimoto's and the scalloped colloid in Graves'.
To keep things organized, here's a quick breakdown of how these two states look clinically.
When you're comparing these two, think of Hyperthyroidism as the body's "fast-forward" button and Hypothyroidism as the "slow-motion" button.
| Feature | Hyperthyroidism (e.g., Graves) | Hypothyroidism (e.g., Hashimoto) |
|---|---|---|
| Metabolic Rate | Increased (Weight loss, heat intolerance) | Decreased (Weight gain, cold intolerance) |
| Skin/Hair | Warm, moist skin; fine hair | Cold, dry skin; brittle hair; loss of outer 1/3 of eyebrows |
| Neuro/Psych | Anxiety, insomnia, tremors, hyperreflexia | Depression, fatigue, mental slowness, hyporeflexia |
| Cardiovascular | Tachycardia, palpitations, atrial fibrillation | Bradycardia, dyspnea on exertion |
| GI | Frequent bowel movements / Diarrhea | Constipation |
| Musculoskeletal | Proximal muscle weakness | Myopathy, carpal tunnel syndrome |
| Labs | Low TSH, High T3/T4 | High TSH, Low T3/T4 |
Now, let's look at the two most common autoimmune causes for these states:
Graves' Disease (Hyperthyroidism)
- Pathophysiology: A Type II Hypersensitivity reaction where the body produces Thyroid-Stimulating Immunoglobulins (TSI). These antibodies mimic TSH and constantly stimulate the TSH receptor.
- Unique Features:
- Exophthalmos (bulging eyes) due to fibroblast proliferation and osmotic swelling behind the eyes.
- Pretibial Myxedema (waxy, orange-peel skin on the shins).
- Diagnosis: Low TSH, High T4, and a diffuse, high uptake on a radioactive iodine scan.
Hashimoto's Thyroiditis (Hypothyroidism)
- Pathophysiology: The most common cause of hypothyroidism in iodine-sufficient regions. It involves autoimmune destruction of the gland by anti-TPO (thyroid peroxidase) and anti-thyroglobulin antibodies.
- Histology: Look for lymphocytic infiltrates with germinal centers and Hürthle cells (eosinophilic, granular cytoplasm).
- Key Risk: Patients have an increased risk of developing Non-Hodgkin B-cell lymphoma (specifically Marginal Zone Lymphoma).
- Clinical Course: May start with a transient hyperthyroid phase ("Hashitoxicosis") as stored hormones leak out of the dying cells, but it ultimately leads to permanent hypothyroidism.
I'll pull up some lessons and flashcards so you can dive deeper into the management and specific lab patterns!
📚 Thyroid Disorder Lessons
Those lessons cover everything from the basic pathology to the clinical management. To help you lock in these facts—especially the antibody names and histological findings—let's look at some flashcards.
🗂️ Thyroid Flashcards
Tap to study 33 flashcards in the Oncourse app
Those flashcards are perfect for drilling the high-yield histology—especially those germinal centers and Hürthle cells for Hashimoto's.
One last pro-tip for your exams: if you see a patient with hyperthyroidism symptoms but a painful, tender thyroid after a viral illness, think Subacute Granulomatous (de Quervain) Thyroiditis. It's a classic "distractor" for Graves' disease!
Do you want to try a quick quiz to see how these concepts show up in clinical cases, or should we look at the management of these conditions?
Setting up chat...