Testicular torsion: diagnosis, bell clapper deformity and surgical management
Testicular torsion is a true urological emergency where the spermatic cord twists, cutting off the blood supply to the testicle. It's a "race against the clock" situation because every hour counts when it comes to saving the gland.
I'll start by finding some visual aids to help illustrate the anatomy and the specific deformity involved.
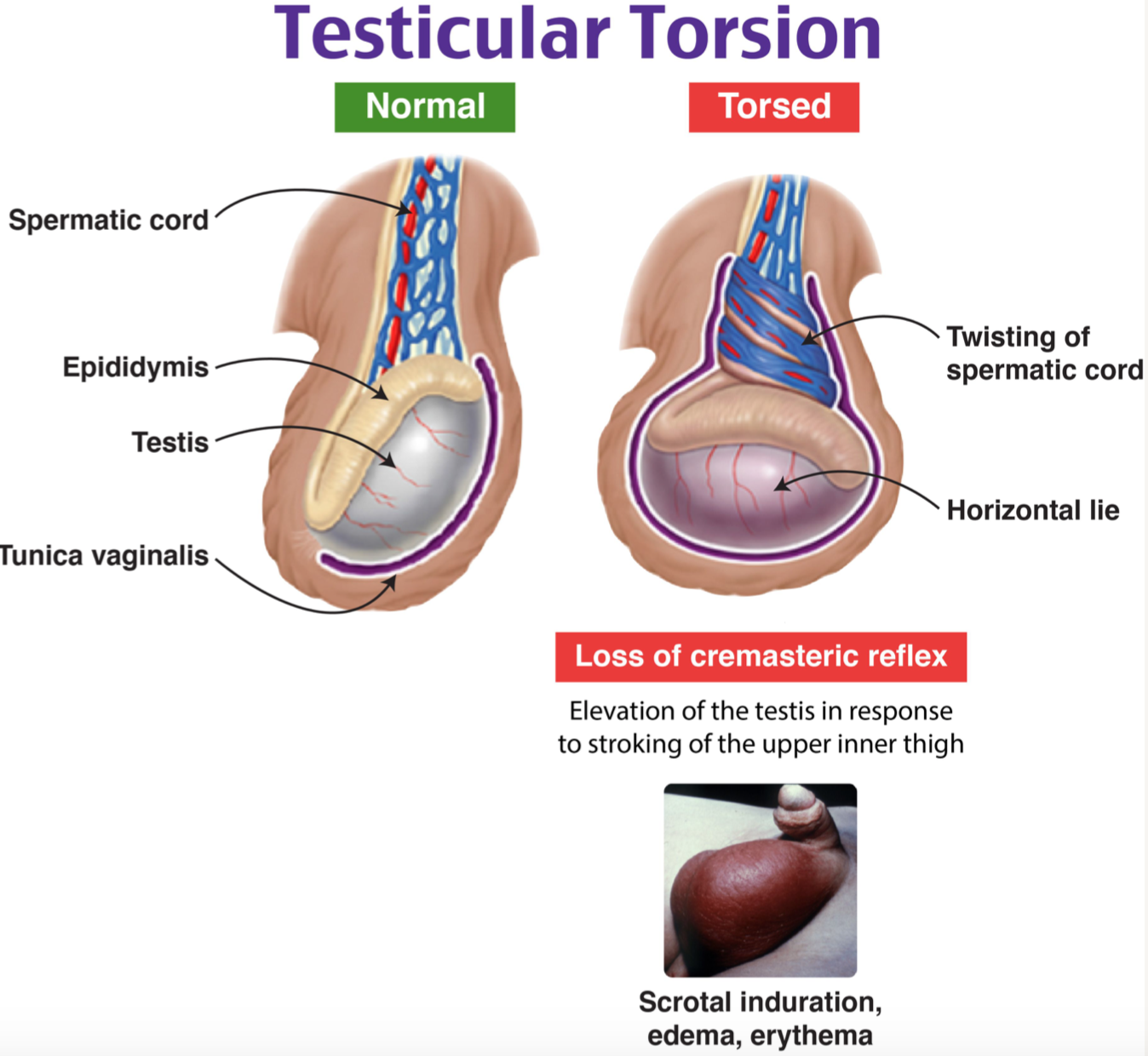
The image below perfectly illustrates the difference between a normal testis and one undergoing torsion, highlighting that characteristic "horizontal lie."
The Bell Clapper Deformity
Normally, the tunica vaginalis covers the testis and epididymis except at the posterior aspect, where they are attached to the scrotal wall. In the bell clapper deformity, the tunica vaginalis completely surrounds the testis, epididymis, and spermatic cord. This allows the testis to hang freely and rotate within the tunica like a clapper inside a bell. This is usually a bilateral anatomical variant, which is why we always treat both sides!
Diagnosis
Diagnosis is primarily clinical. If you suspect it, you call the surgeons immediately.
- Presentation: Sudden onset, severe unilateral scrotal pain, often associated with nausea and vomiting.
- Physical Exam:
- High-riding testis: The affected side sits higher than the other.
- Horizontal lie: Instead of vertical, the testis sits sideways.
- Absent Cremasteric Reflex: ==This is the most sensitive physical finding.== If you stroke the inner thigh and the testis doesn't move up, torsion is highly likely.
- Prehn's Sign: Negative (lifting the scrotum does not relieve pain, unlike in epididymitis).
- Imaging: Color Doppler Ultrasound is the gold standard if the diagnosis is uncertain. It will show decreased or absent blood flow. However, never delay surgery for an ultrasound if the clinical suspicion is high.
Surgical Management
This is a surgical emergency. The goal is to restore blood flow within 6 hours to have the best chance of saving the testis (salvage rate drops significantly after 12-24 hours).
- Exploration: A scrotal incision is made to reach the affected testis.
- Detorsion: The cord is untwisted.
- Assessment of Viability: The testis is wrapped in warm saline-soaked gauze for a few minutes. If it regains color, it's viable. If it remains black/necrotic, an orchidectomy (removal) is performed.
- Orchiopexy: If viable, the testis is fixed to the scrotal wall with non-absorbable sutures to prevent recurrence.
- Contralateral Orchiopexy: Because the bell clapper deformity is usually bilateral, the other side is also fixed during the same procedure to prevent future torsion.
Let's look at the clinical pathway for managing a patient with an acute scrotum.
That flowchart should give you a clear path for management. Remember, the key takeaway is that clinical suspicion alone is enough to warrant surgery.
To help you dive deeper into this topic and lock in these high-yield facts, I've pulled up some relevant lessons and flashcards for you.
🗂️ Testicular Torsion Flashcards
Tap to study 21 flashcards in the Oncourse app
📚 Testicular Torsion Lessons
I've linked some high-yield lessons and flashcards above that cover everything from the initial presentation to the surgical steps.
One last clinical pearl: if you're ever in a situation where surgery is delayed (like during transport), you can attempt manual detorsion. The classic teaching is the "opening a book" maneuver—rotating the testis from medial to lateral. However, this is just a temporary measure and doesn't replace the need for definitive surgery and orchiopexy!
Do you want to try a quick clinical case to see how you'd handle a patient presenting with these symptoms?
Setting up chat...