Stroke: FAST assessment, thrombolysis criteria and acute management pathway
Stroke is a massive topic for the UKMLA AKT, and getting the acute management right is absolutely high-yield. It's all about "time is brain," so let's break down the initial assessment and the pathway you'll need to know for the wards and the exam.
The FAST Assessment
The FAST tool is the gold standard for rapid bedside screening to identify a potential stroke:
- F - Facial weakness: Can the patient smile? Is there any drooping of the mouth or eye?
- A - Arm weakness: Can the patient raise both arms and keep them there?
- S - Speech problems: Is their speech slurred or garbled? Can they understand you?
- T - Time to call 999: If any of these signs are present, it’s an emergency.
In the hospital, we often use the ROSier scale (Recognition of Stroke in the Emergency Room) to differentiate stroke from "stroke mimics" like hypoglycemia or seizures.
Let me pull up a clear management pathway to show you exactly how the workflow looks from the moment they hit the front door.
This algorithm highlights the critical decision points, especially the "Last Known Well" time and the use of imaging to rule out hemorrhage before any intervention.
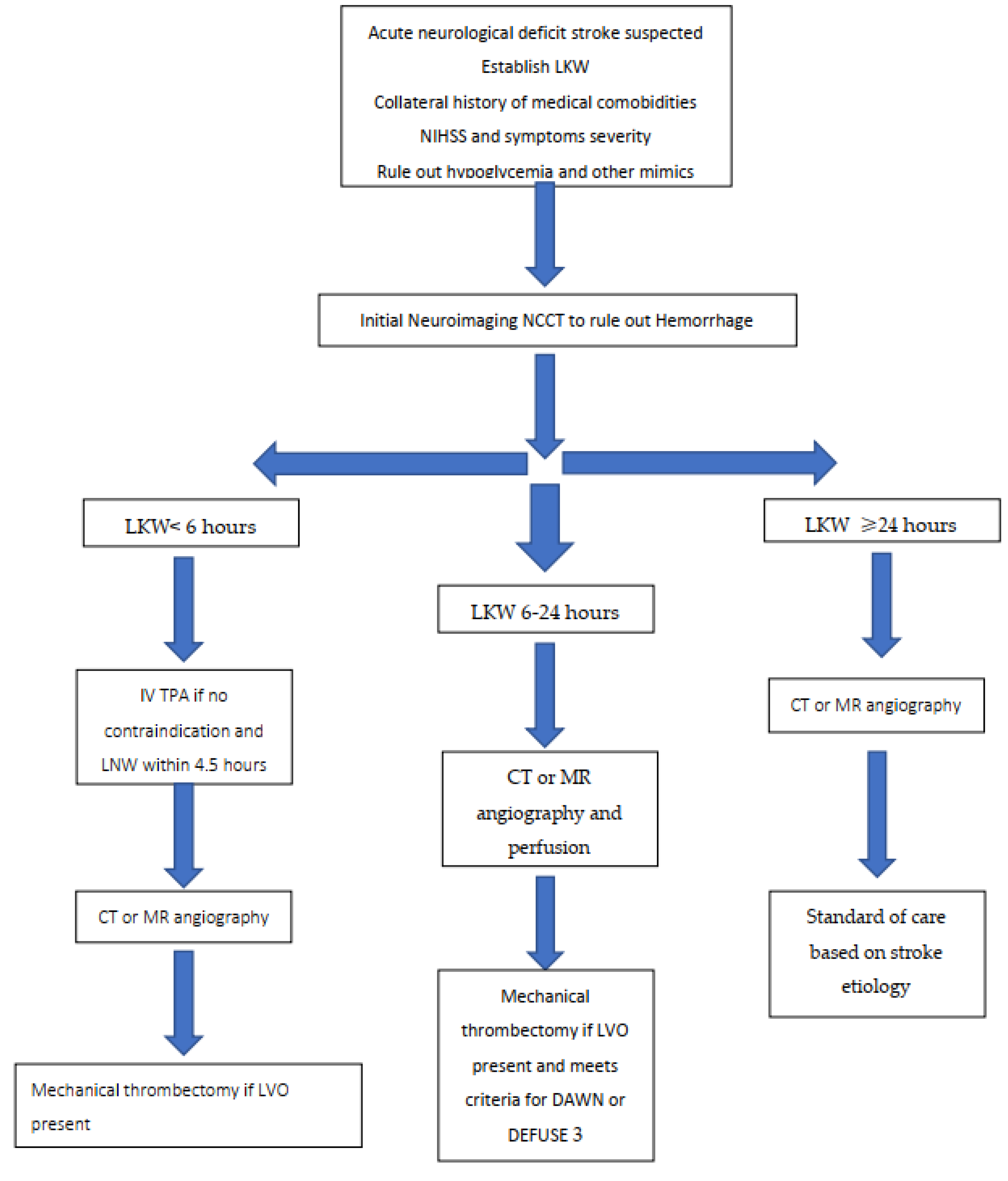
The most critical part of the acute pathway is determining if the patient is a candidate for thrombolysis (usually with Alteplase). In the UK, the window is generally 4.5 hours from the onset of symptoms.
Here is a breakdown of the criteria you'll need to remember:
| Criteria Type | Details |
|---|---|
| Inclusion | Clinical diagnosis of ischemic stroke with measurable neurological deficit (NIHSS score). |
| Time Window | Symptoms started < 4.5 hours ago (some centers extend this with advanced imaging). |
| Absolute Contraindications | Intracranial hemorrhage on CT, previous ICH, major surgery in last 14 days, recent GI/urinary bleed (21 days), platelet count < 100,000, or current use of anticoagulants with elevated INR/PTT. |
| Relative Contraindications | Pregnancy, seizure at onset, minor/improving symptoms, or very high BP (>185/110 mmHg) that cannot be controlled. |
To help you lock this in for the AKT, I've pulled some high-yield lessons and flashcards on stroke management. These will cover the finer details like mechanical thrombectomy (the 6-hour window) and secondary prevention (antiplatelets and statins).
📚 Stroke Management Lessons
Flashcards are great for memorizing those tricky contraindications and time windows. Let's get some for you.
🗂️ Stroke Flashcards
Tap to study 1 flashcard in the Oncourse app
To wrap it up, here’s the quick-fire acute pathway for your exam:
- Initial Assessment: FAST screen and ABCDE. Check blood glucose (rule out hypoglycemia!).
- Imaging: Urgent non-contrast CT head (aim for <1 hour) to rule out hemorrhage.
- Thrombolysis: If ischemic stroke and within 4.5 hours (Alteplase).
- Thrombectomy: Consider if large vessel occlusion (LVO) and within 6 hours (up to 24 hours in specific cases).
- Aspirin: 300mg (after hemorrhage is ruled out) for 2 weeks.
- Admission: To a specialist Hyperacute Stroke Unit (HASU).
High-Yield Tip: For the AKT, remember that blood pressure should only be lowered acutely if it's >220/120 mmHg unless the patient is a candidate for thrombolysis, in which case it must be <185/110 mmHg.
Let me know if you'd like to try a quick quiz on this or if you want to dive into the secondary prevention (like AF and anticoagulation)!
Setting up chat...