Systemic lupus erythematosus: diagnostic criteria, ANA and management
Ah, SLE—the ultimate "great imitator" in medicine! It's a classic for the UKMLA AKT because it can affect literally any organ system, making it a diagnostic challenge. Let me grab some high-yield lessons to get us started on the essentials.
📚 SLE High-Yield Lessons
When we talk about diagnosing SLE, we have to start with the Antinuclear Antibody (ANA) test. Think of it as the "gatekeeper"—it's incredibly sensitive (about 95-99%), so if it's negative, SLE is very unlikely. However, it's not very specific, as it can be positive in other autoimmune conditions or even healthy people.
The 2019 ACR/EULAR criteria actually require a positive ANA (titer ≥1:80) as an entry criterion. Once that's met, you look for clinical and immunological features, each assigned a weight. You need a total score of 10 or more to classify it as SLE. Let me find a good summary of those diagnostic criteria for you.
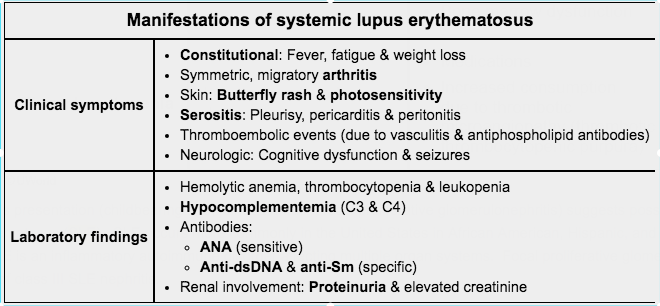
Here is a breakdown of the clinical and immunological features we look for in SLE. Remember, the ANA is the entry point, but more specific antibodies like anti-dsDNA and anti-Smith are the "smoking guns" for diagnosis.
Management of SLE
Management is all about controlling flares and preventing long-term organ damage. Here’s the high-yield breakdown:
1. Lifestyle & Prevention
- Sun Protection: UV light is a major trigger for flares. High-factor sunscreen and protective clothing are essential.
- Cardiovascular Risk: SLE is a pro-inflammatory state, so managing BP, lipids, and smoking is crucial.
2. Pharmacological Management
- Hydroxychloroquine (HCQ): The "gold standard." Almost every patient with SLE should be on HCQ unless contraindicated. It reduces flares, improves survival, and protects the kidneys.
- Exam Tip: Patients on long-term HCQ need annual ophthalmology screening for retinopathy.
- Corticosteroids: Used for acute flares (oral or IV) to get inflammation under control quickly. The goal is always to taper to the lowest effective dose.
- Immunosuppressants: For moderate-to-severe disease or "steroid-sparing" effects:
- Azathioprine: Often used for maintenance.
- Mycophenolate Mofetil (MMF): Preferred for Lupus Nephritis.
- Cyclophosphamide: Reserved for severe, organ-threatening, or life-threatening flares.
- Biologics: Belimumab or Rituximab may be used in refractory cases that don't respond to standard therapy.
Mnemonic: SOAP BRAIN MD (The classic ACR criteria) Serositis, Oral ulcers, Arthritis, Photosensitivity, Blood (cytopenias), Renal (proteinuria), ANA positive, Immunologic (dsDNA/Sm), Neurologic, Malar rash, Discoid rash.
Does that help clear up the diagnostic approach and management for your AKT prep?
Setting up chat...