Shoulder pathology: rotator cuff, frozen shoulder and dislocation management
Shoulder pathology is a bread-and-butter topic for the UKMLA AKT, and it's all about distinguishing between these three based on the patient's age and their specific range of motion. Let's break down the "big three" so you can spot them instantly in a clinical vignette.
1. Rotator Cuff Pathology
This usually presents in older patients or those with repetitive overhead activities. It ranges from impingement/tendinopathy to full-thickness tears.
- Key Sign: Painful arc (pain between
60-120 degreesof abduction). - Rotator Cuff Tear: Weakness in specific movements (e.g., weak external rotation for Infraspinatus).
- Management: Conservative first (physio, NSAIDs) unless it's an acute traumatic tear in a young person, which might need surgery.
2. Frozen Shoulder (Adhesive Capsulitis)
Think of this as a "global" restriction. It’s particularly common in patients with Diabetes Mellitus.
- Key Sign: ==Loss of both active AND passive movement==, especially external rotation.
- Phases: Painful phase -> Stiffening phase -> Thawing phase.
- Management: It's self-limiting but can take up to 2 years. Physio and steroid injections are common.
3. Shoulder Dislocation
95% are Anterior (arm is abducted and externally rotated). Posterior dislocations are rare but classic for AKT questions involving ==seizures or electric shocks== (arm is adducted and internally rotated).
- Management: Urgent reduction under sedation/analgesia.
- Complications: Check the Axillary nerve (sensation over the "regimental badge" area).
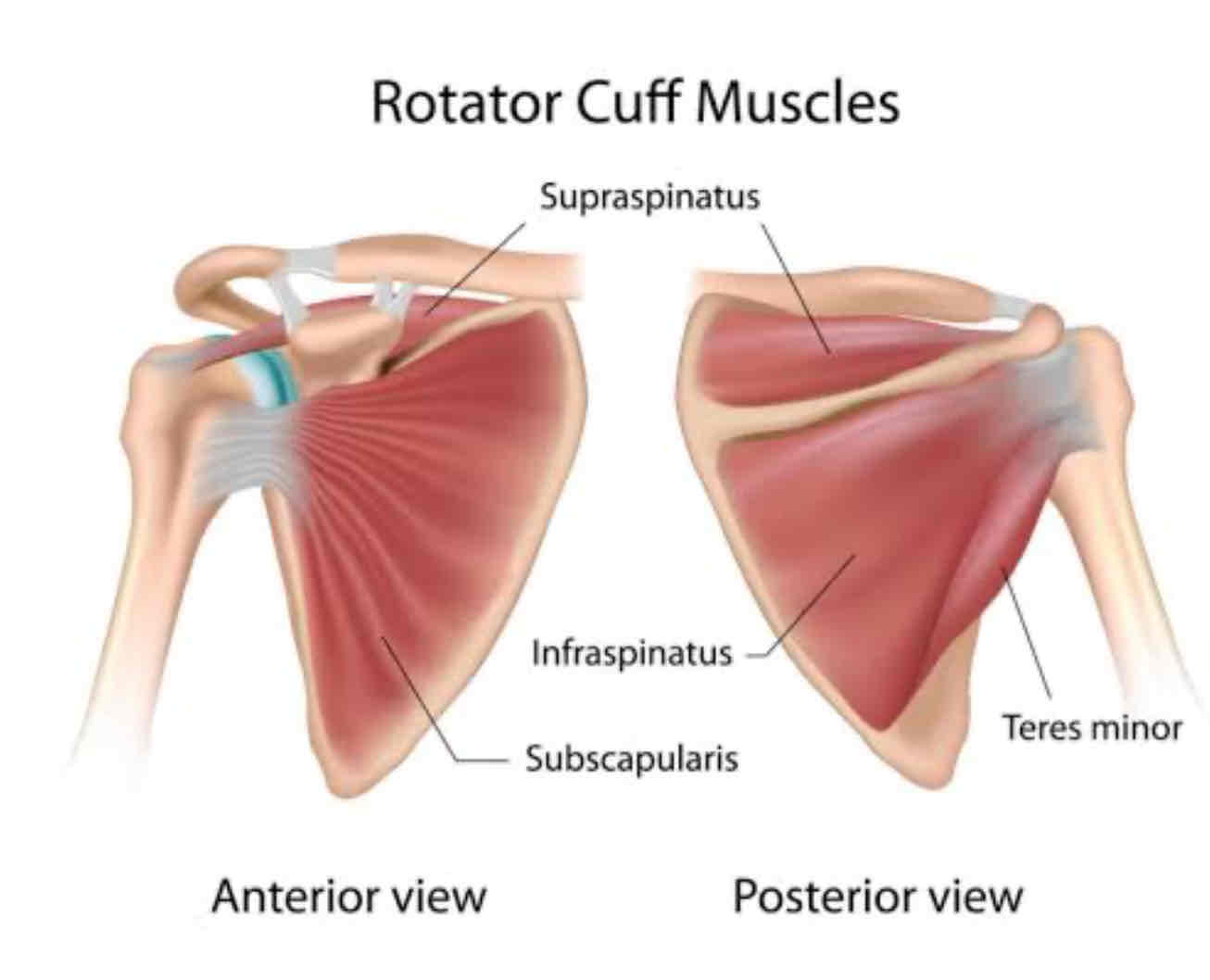
To help you visualize the anatomy we're talking about, let me pull up a diagram of the rotator cuff muscles.
That diagram perfectly shows the SITS muscles (Supraspinatus, Infraspinatus, Teres minor, and Subscapularis). Remember, the Supraspinatus is the one most commonly involved in impingement and tears.
To make your revision easier, I've put together a quick comparison table of these conditions.
| Feature | Rotator Cuff Tear/Impingement | Frozen Shoulder (Adhesive Capsulitis) | Shoulder Dislocation |
|---|---|---|---|
| Typical Patient | Older, overhead athletes | Diabetics, middle-aged | Young (trauma), Elderly (falls) |
| Pain Pattern | Painful arc (60-120°), night pain | Constant dull ache, severe at night | Acute, severe pain after trauma |
| Range of Motion | Active restricted, Passive normal | Both Active & Passive restricted | Unable to move arm; fixed position |
| Key Sign | Weakness in specific tests (e.g. Empty Can) | Loss of external rotation is earliest sign | Squared-off shoulder appearance |
| Management | Physio, NSAIDs, Surgery (if acute) | Self-limiting, Steroid injections, Physio | Reduction, Sling, Axillary nerve check |
📚 Shoulder Pathology Lessons
That table is your "cheat sheet" for the AKT. If you see "passive movement restricted", your mind should immediately jump to Frozen Shoulder. If passive movement is fine but they can't lift their arm themselves, think Rotator Cuff.
I've also pulled up some high-yield lessons on upper limb trauma and clinical correlations that cover these in even more depth.
Since these three conditions are so easy to mix up, would you like to try a quick game of Synapses to see if you can group the clinical features correctly? Or we could jump straight into some practice questions!
Setting up chat...