Rheumatoid arthritis: diagnosis, DMARDs and biologic therapy
Rheumatoid Arthritis (RA) is a absolute staple for the UKMLA AKT. The key thing to remember for the exam is the "treat-to-target" strategy—we want to get patients into remission as fast as possible to prevent permanent joint damage.
1. Diagnosis: Catching it Early
In the UK, NICE guidelines (NG100) emphasize urgent referral (within 3 weeks) for anyone with suspected persistent synovitis.
- Clinical Features: Symmetrical, small joint polyarthritis (MCP, PIP, MTP joints). Look for morning stiffness lasting more than 30 minutes.
- Investigations:
- Rheumatoid Factor (RF): Present in about 70-80%, but not specific.
- Anti-CCP (ACPA): Highly specific and often appears before clinical symptoms.
- Imaging: X-rays may show soft tissue swelling early on, progressing to ==periarticular osteopenia, joint space narrowing, and marginal erosions==.
- Monitoring: We use the DAS28 score (Disease Activity Score) to monitor progress and decide on treatment escalation.
Let me find a good visual for the clinical presentation and diagnostic criteria to help lock this in.
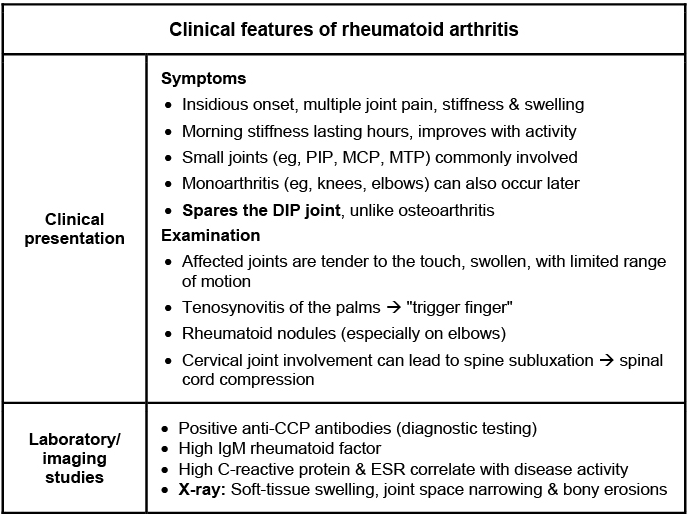
This diagram highlights the classic distribution of RA (sparing the DIP joints!) and the key lab findings like Anti-CCP and RF.
2. Conventional Synthetic DMARDs (csDMARDs)
NICE recommends ==first-line treatment with DMARD monotherapy== (usually Methotrexate) as soon as possible, often with a short course of bridging steroids to get symptoms under control while the DMARD kicks in (which can take 6-12 weeks).
- Methotrexate: The "gold standard." It's a folate antagonist.
- Crucial AKT point: Always co-prescribe Folic Acid (taken on a different day) and monitor for ==pulmonary fibrosis and hepatotoxicity==.
- Sulfasalazine: Safe in pregnancy. Watch for rashes and oligospermia (reversible).
- Hydroxychloroquine: Used for mild disease. Main concern is ==retinopathy== (needs baseline and annual eye screening).
- Leflunomide: Similar efficacy to methotrexate but carries a risk of hypertension and peripheral neuropathy.
I've put together a quick reference table for the monitoring and side effects you'll likely be tested on.
| DMARD | Key Side Effects | Monitoring Requirements |
|---|---|---|
| Methotrexate | Myelosuppression, Liver cirrhosis, Pneumonitis | FBC, LFTs, U&Es (every 1-2 weeks until stable, then 3-monthly) |
| Sulfasalazine | Rash, Heinz body anaemia, Oligospermia | FBC, LFTs (similar schedule to Methotrexate) |
| Hydroxychloroquine | Retinopathy (bull's eye maculopathy) | Baseline and annual ophthalmology review |
| Leflunomide | Hypertension, Hepatotoxicity, Peripheral neuropathy | FBC, LFTs, Blood Pressure monitoring |
3. Biologic Therapy (bDMARDs)
When conventional DMARDs aren't enough, we escalate to biologics. In the UK, the threshold for starting biologics is usually a ==DAS28 score > 5.1 despite 2 conventional DMARDs== (one of which must be Methotrexate).
- TNF-alpha Inhibitors: (e.g., Etanercept, Infliximab, Adalimumab).
- AKT Point: You must screen for ==latent TB and Hepatitis B/C== before starting, as these can reactivate.
- B-cell Depletion: (e.g., Rituximab). Often used if TNF inhibitors fail.
- IL-6 Inhibitors: (e.g., Tocilizumab).
- JAK Inhibitors: (e.g., Tofacitinib, Baricitinib). These are actually "targeted synthetic" (tsDMARDs) and are taken orally, but they're used at the same stage as biologics.
Let me pull up some relevant lessons so you can dive deeper into the specific management pathways and the DAS28 scoring system.
📚 RA Management Lessons
Those lessons cover the management pathways in detail, which is perfect for the AKT.
To wrap up, here's your High-Yield RA Checklist:
- Urgent Referral: Within 3 weeks for suspected persistent synovitis.
- First-line: Methotrexate monotherapy + bridging steroids.
- Monitoring: DAS28 score is the key metric for escalation.
- Biologics: Start if DAS28 > 5.1 despite 2 csDMARDs.
- Safety: Screen for TB before starting TNF inhibitors; monitor FBC/LFTs for Methotrexate.
Since there are so many different drug classes to keep track of, would you like to try a quick game of Synapses to see if you can correctly group the DMARDs and biologics?
Setting up chat...