Psychosis: first episode assessment, antipsychotic choice and side effect comparison
Psychosis can be one of the most challenging but fascinating areas of psychiatry to master for the AKT. When a patient presents with their first episode of psychosis (FEP), the goal is early intervention to improve long-term outcomes.
Let's start by looking at some high-yield lessons that cover the assessment and management of psychosis in detail.
📚 Psychosis Lessons
For the AKT, remember that the assessment of First Episode Psychosis (FEP) is all about ruling out organic causes while identifying the core psychotic symptoms. You'll want to check for:
- History: Focus on hallucinations, delusions, and thought interference. Don't forget to screen for substance use and mood symptoms.
- Physical Exam: A full neurological exam is a must to rule out space-occupying lesions or other neuro conditions.
- Investigations: Baseline bloods are crucial—FBC, U&Es, LFTs, Glucose, Lipids, and TFTs. A urine drug screen is also standard practice.
When it comes to choosing an antipsychotic, NICE guidelines emphasize a shared decision-making process. Since most atypical (second-generation) antipsychotics have similar efficacy for positive symptoms, the choice usually boils down to which side effects the patient wants to avoid most.
I'll pull up a comparison table of the common antipsychotics and their side effect profiles to help you visualize the differences.
| Antipsychotic | Type | Key Side Effects | Clinical Notes |
|---|---|---|---|
| Olanzapine | Atypical | Significant weight gain, metabolic syndrome, sedation | High risk of diabetes and dyslipidemia. |
| Risperidone | Atypical | Hyperprolactinaemia (amenorrhea, galactorrhea), EPS at higher doses | Good all-rounder but watch the prolactin. |
| Quetiapine | Atypical | Sedation, orthostatic hypotension, moderate weight gain | Often used if sleep is a major issue. |
| Aripiprazole | Atypical | Akathisia, insomnia, anxiety | "Dopamine stabilizer"; lowest risk of weight gain/prolactin. |
| Haloperidol | Typical | High risk of Extrapyramidal Side Effects (EPS), tardive dyskinesia | Rarely first-line for FEP now. |
| Clozapine | Atypical | Agranulocytosis, myocarditis, seizures, constipation | Reserved for treatment-resistant schizophrenia (failed 2 others). |
That table covers the big hitters you'll see in the AKT. A common exam trick is to ask about Clozapine—always remember it's for treatment-resistant cases (failed two other antipsychotics, one being an atypical) and requires strict FBC monitoring for agranulocytosis.
For any patient starting an antipsychotic, you'll need to monitor:
- Weight/BMI (weekly for first 6 weeks, then at 12 weeks, 1 year, and annually)
- Blood Pressure & Pulse (at start, 12 weeks, 1 year, and annually)
- HbA1c & Lipids (at start, 12 weeks, 1 year, and annually)
- Prolactin (if symptoms of hyperprolactinaemia occur)
In the UK, anyone with a first episode of psychosis should be referred to an Early Intervention in Psychosis (EIP) service within two weeks.
To help you visualize the different Extrapyramidal Side Effects (EPS) that can occur, let me find a diagram for you.
This diagram is a great summary of the Extrapyramidal Side Effects (EPS) you'll need to know for the AKT. It breaks down the timing and presentation of acute dystonia, akathisia, and tardive dyskinesia, which are classic exam questions.
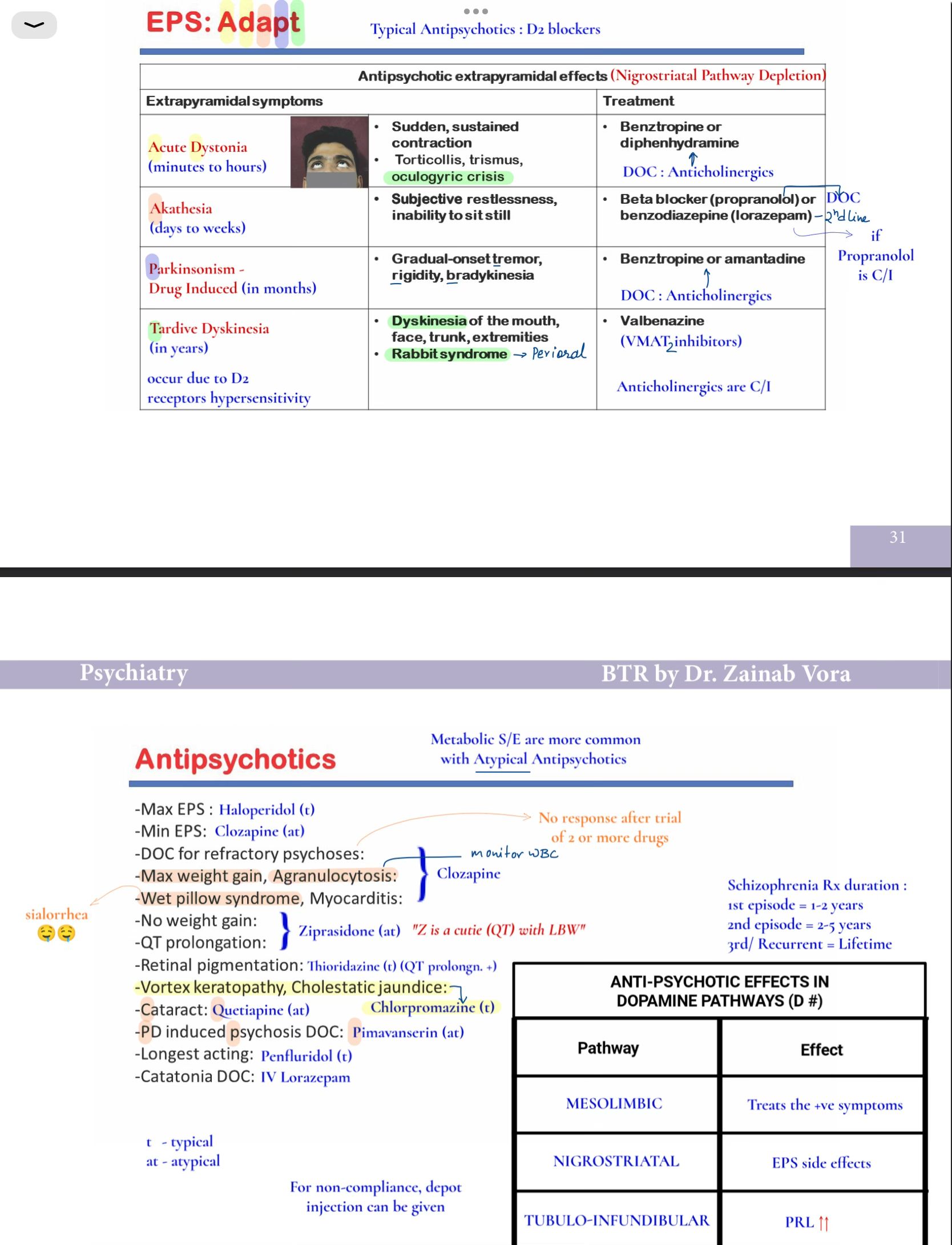
That diagram is a lifesaver for the AKT. A quick mnemonic for the timing of EPS is the "Rule of 4":
- 4 hours: Acute dystonia (e.g., oculogyric crisis)
- 4 days: Akathisia (restlessness)
- 4 weeks: Parkinsonism (tremor, rigidity)
- 4 months: Tardive dyskinesia (involuntary movements)
For the UK exams, always remember that the Early Intervention in Psychosis (EIP) service is the gold standard for anyone aged 14–65 with a first episode of psychosis. They aim to provide a full assessment and start treatment within two weeks of referral.
If you're feeling confident with the theory, we could jump into some practice questions or even a clinical case to see how you'd manage a patient in a real-world scenario!
Setting up chat...