Prescribing in the elderly: polypharmacy review, STOPP/START criteria
Prescribing for the elderly is like a high-stakes game of Jenga—one wrong move and the whole thing can come crashing down! It's a massive topic for the UKMLA AKT because, in the NHS, our patients are getting older and their medication lists are getting longer.
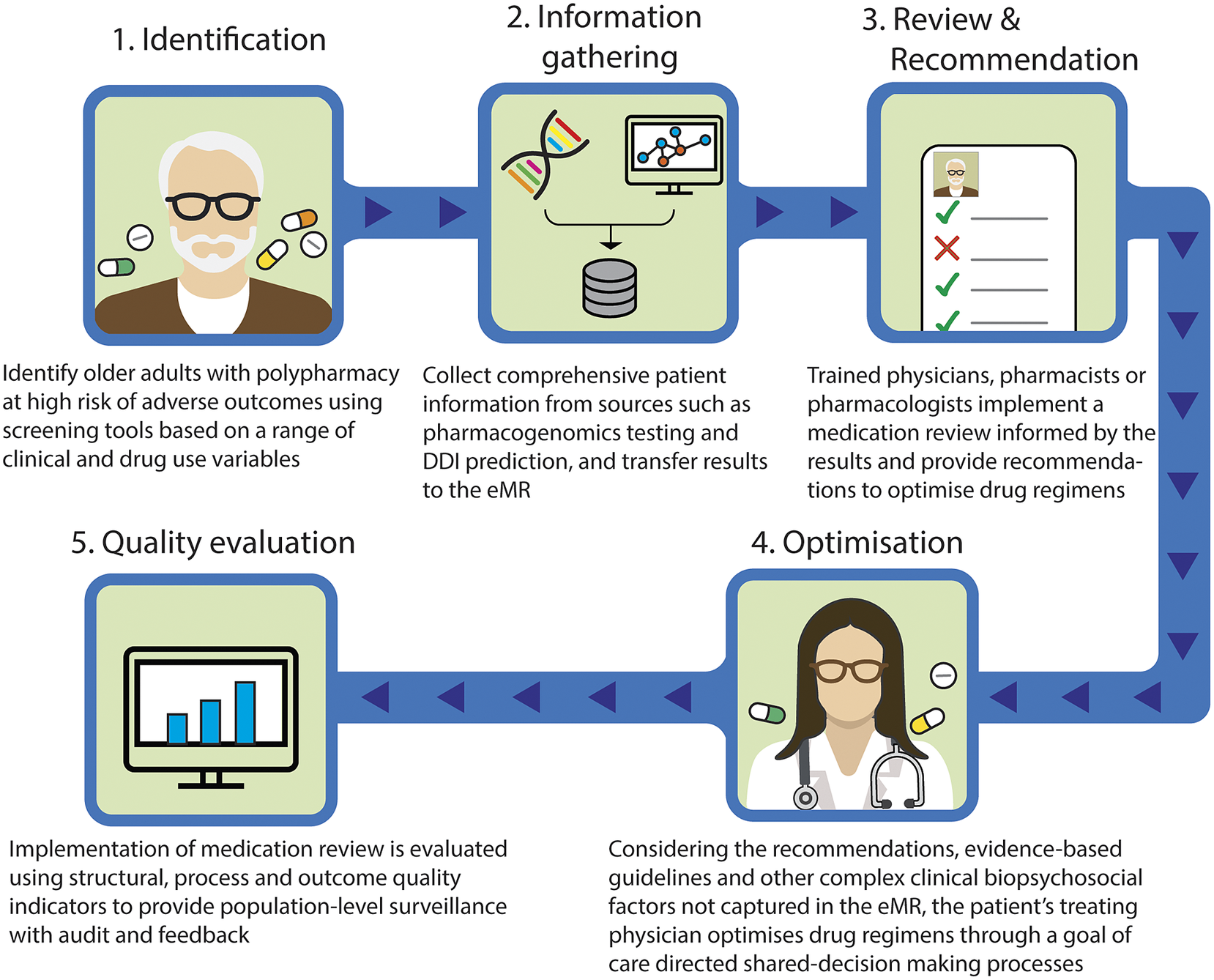
The goal isn't just to "give pills," but to ensure we aren't causing more harm than good through polypharmacy. Let me find a good visual to help us visualize the approach to reviewing these complex medication lists.
That visual gives a great overview of the systematic approach we take. Now, the "gold standard" we use in the UK is the STOPP/START criteria. Think of it as a clinical audit for your patient's pillbox.
- STOPP: Screening Tool of Older Persons' Prescriptions (what to stop to avoid PIMs—Potentially Inappropriate Medicines).
- START: Screening Tool to Alert to Right Treatment (what to start that we might be missing).
Here's a quick breakdown of the high-yield examples you'll likely see in exam questions.
| Category | STOPP (Stop these!) | START (Start these!) |
|---|---|---|
| Cardiovascular | Digoxin >125mcg/day (if renal impairment) | ACEi in Heart Failure |
| CNS | Benzodiazepines (falls risk!) | SSRIs for persistent depression |
| Gastro | Long-term PPIs (unless high risk) | Laxatives for opioid-induced constipation |
| Musculoskeletal | NSAIDs with Warfarin/DOACs | Bisphosphonates in chronic steroid use |
| Endocrine | Glibenclamide (long-acting sulfonylureas) | Statins in DM with high CV risk |
That table covers the "bread and butter" of geriatric prescribing for the AKT. Remember the prescribing cascade—where a new drug is prescribed to treat the side effect of an old one (e.g., Amlodipine causing ankle edema, so Furosemide is added).
I've got some great lessons that dive deeper into the specifics of geriatric prescribing and the physiological changes (like reduced GFR and increased body fat) that make these drugs so tricky.
📚 Geriatric Prescribing Lessons
Since this is a lot of "if this, then that" logic, flashcards are your best friend for memorizing the specific criteria. Let me pull those up for you so you can lock in these high-yield facts.
🗂️ Prescribing Flashcards
Tap to study 11 flashcards in the Oncourse app
Those flashcards will help you nail the specific drug-drug interactions. One final tip for your AKT: always look for anticholinergic burden. Drugs like amitriptyline, oxybutynin, and even some antihistamines can cause confusion, dry mouth, and urinary retention in the elderly.
If you see a patient with new-onset confusion or falls, the first thing you should do is review that med list! You've got this—geriatric medicine is all about the big picture.
Setting up chat...