Pre-eclampsia: diagnostic criteria, NICE management and when to deliver
Pre-eclampsia is a classic "exam favorite" because it involves clear diagnostic criteria and very specific management steps. Since you're prepping for the UKMLA AKT, we'll stick strictly to the NICE guidelines (NG133).
1. Diagnostic Criteria
Pre-eclampsia is defined as new-onset hypertension (occurring after 20 weeks of gestation) plus one or more of the following:
- Proteinuria: Protein/creatinine ratio (PCR) of
30 mg/mmolor more, or a 24-hour urine protein of0.3 gor more. - Organ dysfunction: Such as renal impairment (creatinine
>90 μmol/L), hepatic involvement (elevated ALT/AST), or neurological complications (e.g., eclampsia, severe headache, visual scotomata). - Uteroplacental dysfunction: Such as fetal growth restriction (FGR).
Note: Hypertension is defined as a systolic BP
≥140 mmHgor diastolic BP≥90 mmHg.
2. NICE Management Guidelines
Management focuses on controlling blood pressure and monitoring for complications.
Antihypertensive Choice:
- Labetalol: First-line (unless the patient has asthma).
- Nifedipine (modified-release): Second-line.
- Methyldopa: Third-line.
Prophylaxis (The "Aspirin Rule"):
Women at high risk should take 75–150 mg of Aspirin daily from 12 weeks until birth.
- High risk (1 factor needed): Hypertensive disease in previous pregnancy, chronic kidney disease, autoimmune disease (SLE/APS), Type 1 or 2 diabetes, or chronic hypertension.
- Moderate risk (2 factors needed): First pregnancy, age
≥40, pregnancy interval>10 years, BMI≥35 kg/m², or family history of pre-eclampsia.
3. When to Deliver?
The timing of delivery is a balance between fetal maturity and maternal/fetal safety.
- Pre-eclampsia (Stable): Delivery is usually recommended at 37 weeks.
- Severe Pre-eclampsia: If BP cannot be controlled (
>160/110 mmHg) or there is evidence of maternal/fetal deterioration (e.g., HELLP syndrome, rising creatinine, or abnormal CTG), delivery is often indicated regardless of gestational age, usually after a course of corticosteroids.
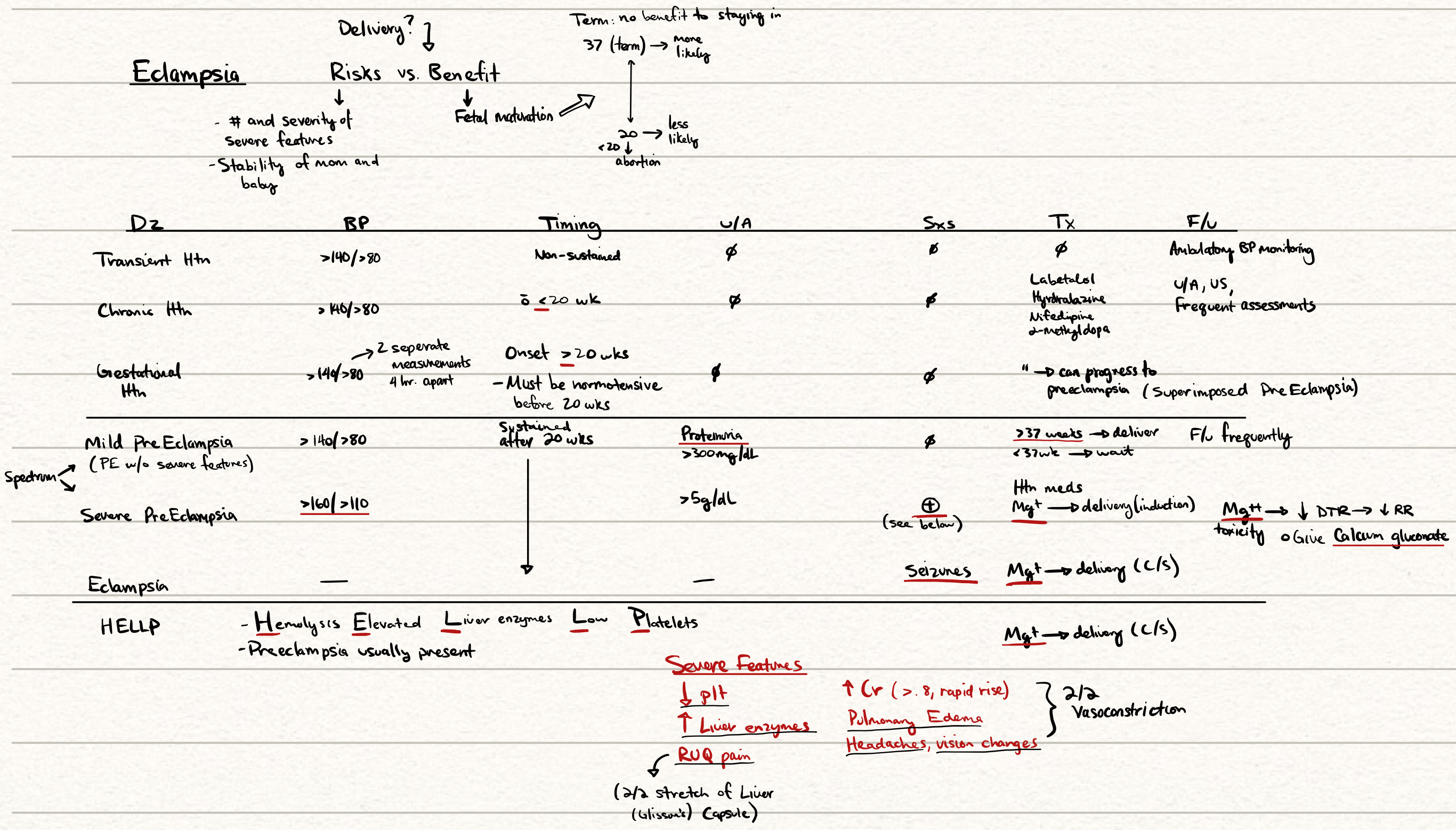
I'll pull up a management algorithm to help you visualize the clinical pathway for hypertension in pregnancy.
This diagram provides a great overview of the different hypertensive disorders in pregnancy, including the specific thresholds for severe pre-eclampsia and the HELLP syndrome triad.
I've also found some high-yield lessons that cover the NICE guidelines in more detail, specifically focusing on the UKMLA AKT requirements.
📚 Pre-eclampsia Lessons
To help you lock in those diagnostic thresholds and the aspirin prophylaxis rules, here are some flashcards for active recall.
🗂️ Pre-eclampsia Flashcards
Tap to study 16 flashcards in the Oncourse app
Pre-eclampsia is one of those topics where the examiners love to test the "numbers"—so keep that 140/90 and 37 weeks threshold in mind!
If you're feeling confident with the theory, I can set up a quick quiz to see how you handle some clinical scenarios, or we could dive into the complications like HELLP syndrome or Eclampsia management. What do you think?
Setting up chat...