Pneumothorax: primary vs secondary, tension pneumothorax and management
Ah, the classic "collapsed lung" scenario! Pneumothorax is a staple for the UKMLA AKT, and keeping the different types straight is key to getting those management questions right.
To start us off, let's look at the fundamental difference between primary and secondary cases.
Primary vs. Secondary Spontaneous Pneumothorax
The main distinction here is whether there's underlying lung disease. Think of it as "healthy lungs vs. struggling lungs."
| Feature | Primary Spontaneous (PSP) | Secondary Spontaneous (SSP) |
|---|---|---|
| Underlying Lung Disease | None (typically tall, thin young men) | Present (e.g., COPD, Asthma, CF, Fibrosis) |
| Risk Factors | Smoking, family history | Age >50, significant smoking history, existing lung pathology |
| Pathophysiology | Rupture of subpleural blebs | Complication of existing disease |
| Management Threshold | More conservative | More aggressive (lower threshold for intervention) |
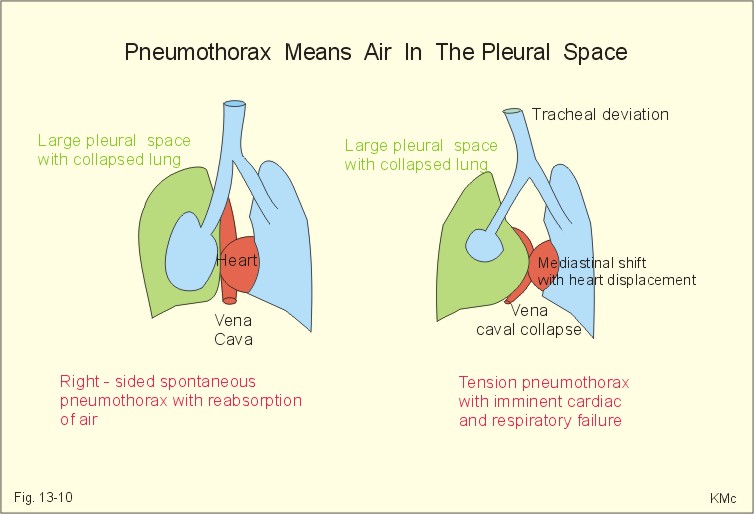
I'll pull up a diagram so you can visualize what's actually happening in the pleural space.
This diagram perfectly illustrates the difference between a standard pneumothorax and the life-threatening tension variety. Notice the shift in the heart and trachea in the tension example—that's the "red flag" you need to watch for.
Tension Pneumothorax: The Medical Emergency
This is a clinical diagnosis. You don't wait for an X-ray if you suspect this!
- Pathophysiology: A "one-way valve" effect where air enters the pleural space during inspiration but cannot escape during expiration.
- The Result: Intrapleural pressure rises, compressing the lung and eventually the mediastinum. This squashes the superior vena cava, leading to obstructive shock.
- Key Signs:
- Severe respiratory distress.
- Tracheal deviation (away from the affected side).
- Distended neck veins (raised JVP).
- Hyper-resonance on percussion.
- Hypotension (late sign).
Immediate Action: Needle decompression! Insert a large-bore cannula into the 2nd intercostal space, mid-clavicular line (though newer guidelines also suggest the 5th ICS, anterior axillary line). Don't wait for imaging!
Management (BTS Guidelines)
Management depends heavily on whether it's primary or secondary and the size of the rim of air (measured at the level of the hilum).
I've put together a flowchart to help you navigate the British Thoracic Society (BTS) approach, which is what you'll need for the UKMLA.
That flowchart should give you a solid roadmap for the AKT! Remember, the key is to look for that underlying lung disease (COPD is the most common culprit in exams) and the size of the pneumothorax.
I've found some high-yield lessons that go into even more detail on the clinical presentation and the specific BTS guidelines.
📚 Pneumothorax Lessons
Those lessons are excellent for a deep dive into the ATLS protocols and specific cardiothoracic management.
Ready to see if you can spot the tension pneumothorax in a clinical scenario? I can set up a quick quiz for you to practice!
✍️ Pneumothorax Practice Quiz
Tap to practice questions in the Oncourse app
That quiz will really help you nail down the BTS management thresholds.
If you're feeling like a quick break from the standard questions, we could try a game of Synapses to help you categorize the different management steps for primary vs. secondary pneumothorax. It's a great way to make those distinctions stick!
Would you like to try that, or is there anything else about pneumothorax you're curious about?
Setting up chat...