Perioperative medicine: preoperative assessment, cardiac risk and management
Perioperative medicine is such a critical bridge between surgery and internal medicine. Getting the preoperative assessment right is basically the "safety check" that ensures a patient actually makes it off the table and through recovery without major complications.
Let me pull up some high-yield lessons on this topic to give you a solid foundation.
📚 Perioperative Cardiac Risk Lessons
When we talk about cardiac risk, we're usually looking at two main things: the patient's clinical risk factors and the surgical risk itself.
One of the most common tools we use is the Revised Cardiac Risk Index (RCRI), also known as Lee's Criteria. It helps us predict the risk of major adverse cardiac events (MACE).
The RCRI Criteria
Each of these counts as 1 point:
- High-risk surgery (intraperitoneal, intrathoracic, or suprainguinal vascular)
- History of Ischemic Heart Disease (IHD)
- History of Congestive Heart Failure (CHF)
- History of Cerebrovascular Disease (TIA/Stroke)
- Diabetes Mellitus requiring insulin
- Preoperative Creatinine > 2.0 mg/dL
Another big factor is Functional Capacity, measured in METs (Metabolic Equivalents).
- < 4 METs: Poor (Can't climb two flights of stairs or carry groceries)
- > 4 METs: Good (Can do heavy housework or climb stairs without stopping)
If a patient has > 4 METs, they usually don't need further cardiac testing, even if they have risk factors!
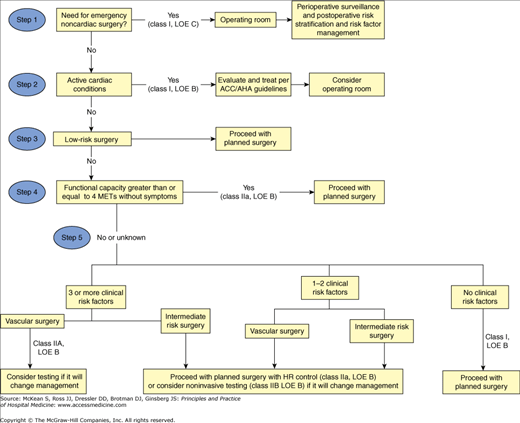
Let me find a visual for the cardiac risk stratification algorithm to make this clearer.
This flowchart from the ACC/AHA guidelines is the gold standard for how we decide if a patient needs more testing or can head straight to the OR.
One of the most common questions on exams is which medications to keep and which to stop. It's a bit of a balancing act between preventing a cardiac event and avoiding intraoperative complications like hypotension or bleeding.
Here's a quick summary of the most important ones:
| Medication | Perioperative Management | Key Reason |
|---|---|---|
| Beta-blockers | Continue if already on them. | Prevents rebound tachycardia/ischemia. |
| Statins | Continue. | Plaque stabilization; reduces MACE. |
| ACE inhibitors / ARBs | Hold 24 hours before surgery. | High risk of intraoperative hypotension. |
| Diuretics | Hold on the morning of surgery. | Risk of hypovolemia and electrolyte shifts. |
| Aspirin | Continue for high-risk cardiac patients. | Stop only for high-bleeding risk (e.g., neurosurgery). |
| Clopidogrel | Stop 5-7 days before surgery. | High bleeding risk. |
| Warfarin | Stop 5 days before; bridge with LMWH if high risk. | Normalize INR for surgery. |
| Oral Hypoglycemics | Hold on the morning of surgery. | Risk of hypoglycemia while NPO. |
| Insulin | Reduce dose (usually 50-75% of basal). | Prevent hypoglycemia while NPO. |
One last thing to keep in mind is the timing of surgery after cardiac interventions. This is a classic exam question!
- Balloon Angioplasty: Wait 14 days before elective surgery.
- Bare Metal Stent (BMS): Wait 30 days before elective surgery.
- Drug-Eluting Stent (DES): Wait 6 months (ideally 12 months) before elective surgery.
If you go in too early, the risk of stent thrombosis is sky-high!
Would you like to test your knowledge with a quick quiz on these perioperative cardiac risk factors?
✍️ Perioperative Cardiac Risk Quiz
Tap to practice questions in the Oncourse app
I've set up a quiz for you to test your knowledge on these perioperative cardiac risk factors. It's a great way to see if you've got the RCRI and medication management down!
If you want to try something a bit more interactive, we could play a game of Synapses to categorize which medications to Continue vs. Hold on the morning of surgery. It's a fun way to lock in those high-yield facts.
What do you think? Ready for the quiz or want to try the game first?
Setting up chat...