Pediatric cardiology: congenital heart diseases classification and management
Pediatric cardiology can feel like a bit of a maze with all the different shunts and "T" names, but it's actually quite logical once you break it down by how the blood flows!
To get us started, I'll pull up some of the best lessons we have on the classification and management of these conditions so you have a solid foundation to work from.
The most common way we classify Congenital Heart Disease (CHD) is based on whether the baby looks "blue" (cyanotic) or "pink" (acyanotic). It all comes down to where the blood is shunting!
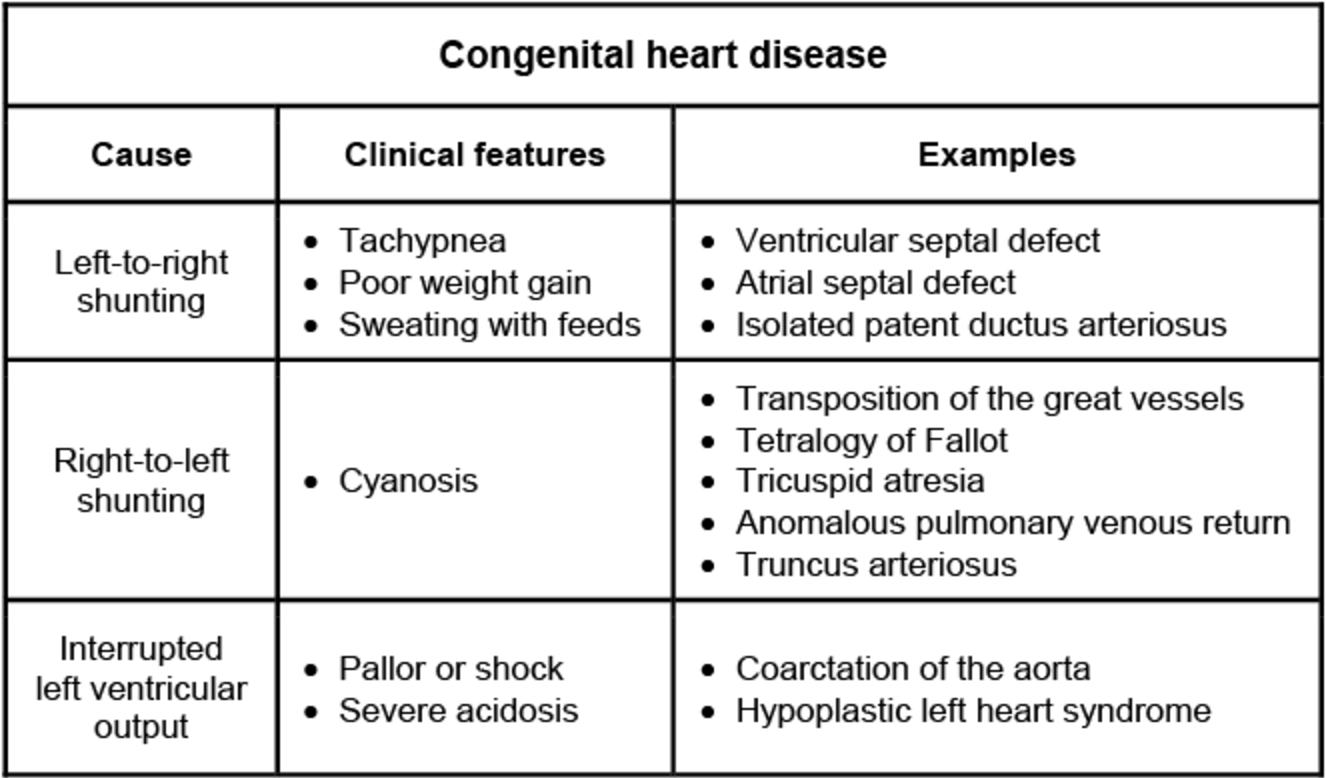
I'm going to find a clear comparison table or diagram that breaks these down by their pathophysiology, as this is a very high-yield way to remember them for exams.
This table is a perfect summary of how these defects present clinically. Notice how the Left-to-Right shunts (like VSD and ASD) usually lead to heart failure symptoms like tachypnea and poor feeding, while the Right-to-Left shunts (the "T" diseases) are where you'll see that classic cyanosis.
When it comes to management, we usually think in three phases: medical stabilization, interventional procedures, and definitive surgery.
1. Medical Management
- Prostaglandin E1 (PGE1): This is the "emergency" drug for duct-dependent lesions (like TGA, severe Coarctation, or HLHS). It keeps the Ductus Arteriosus open to allow for life-saving mixing of blood.
- Heart Failure Support: For large left-to-right shunts (VSD, PDA), we use
Diuretics(Furosemide) and sometimesDigoxinto manage pulmonary congestion. - PDA Closure: In premature infants, we use
IndomethacinorIbuprofen(NSAIDs) to help close a patent ductus.
2. Interventional Procedures
- Rashkind Procedure: A balloon atrial septostomy done in the cath lab to create an ASD for mixing in TGA.
- Device Closures: Many ASDs and some VSDs can now be closed with a "plug" (Amplatzer device) without open-heart surgery.
3. Surgical Management
- Palliative: The Modified Blalock-Taussig (BT) Shunt is the classic example—it connects the subclavian artery to the pulmonary artery to increase blood flow to the lungs in cyanotic babies (like those with TOF).
- Definitive:
- Arterial Switch (Jatene) for TGA.
- VSD Repair with a patch.
- Fontan Procedure for single ventricle physiology (like Tricuspid Atresia).
High-Yield Tip: If you see a newborn with cyanosis that doesn't improve with 100% oxygen (failed hyperoxia test), think of a cyanotic CHD!
Would you like to try a few practice questions on these, or should we dive deeper into a specific defect like Tetralogy of Fallot?
Setting up chat...