Obstetric emergencies: eclampsia, cord prolapse and shoulder dystocia
Obstetric emergencies are some of the most high-pressure scenarios you'll face in clinical practice. For the UKMLA AKT, you really need to know the immediate "crash call" steps for each of these.
Let's break down the "big three" you mentioned: Eclampsia, Cord Prolapse, and Shoulder Dystocia.
1. Eclampsia
This is defined as one or more convulsions occurring in the context of pre-eclampsia. It’s a true multi-system emergency.
- Immediate Management:
- ABCDE approach: Secure the airway and give high-flow oxygen.
- Stop the seizure: The drug of choice is Magnesium Sulfate (MgSO4).
- Loading dose:
4g IV over 5-10 minutes. - Maintenance:
1g/hour infusion for 24 hoursafter the last seizure.
- Loading dose:
- Blood Pressure: Control with IV Labetalol or Hydralazine if needed.
- Delivery: Once the mother is stable, the definitive treatment is delivery of the baby.
2. Cord Prolapse
This happens when the umbilical cord descends below the presenting part after the membranes have ruptured. The danger here is cord compression leading to fetal hypoxia.
- Key Signs: Sudden fetal bradycardia or decelerations on CTG after Rupture of Membranes (ROM).
- Immediate Actions:
- Call for help (Obstetric emergency call).
- Relieve pressure: Manually push the presenting part (e.g., the head) back up into the pelvis.
- Positioning: Place the mother in the knee-chest position or Trendelenburg (head down).
- Avoid handling the cord: This can cause vasospasm.
- Delivery: Aim for immediate Category 1 Caesarean Section.
3. Shoulder Dystocia
This occurs when the anterior fetal shoulder becomes impacted against the maternal symphysis pubis.
- The "Turtle Sign": The fetal head retracts back against the perineum.
- Management (The HELPERR Mnemonic):
- H - Help (Call for senior obs, paeds, and anaesthetics).
- E - Evaluate for Episiotomy (to allow more room for internal maneuvers).
- L - McRoberts Maneuver: Flex and abduct the maternal hips (this is the first-line move!).
- P - Suprapubic Pressure (to push the shoulder under the bone).
- E - Enter (Internal maneuvers like the Wood’s Screw).
- R - Remove the posterior arm.
- R - Roll the patient onto all fours.
I'll pull up some high-yield lessons and a flowchart to help you visualize these management steps, as they are very common AKT topics!
📚 Obstetric Emergency Lessons
I've found some excellent resources for you. The lessons cover the specific management protocols for each emergency, and I've pulled a great visual for the shoulder dystocia algorithm.
For the AKT, remember that the McRoberts maneuver and suprapubic pressure are the most successful first-line steps for shoulder dystocia.
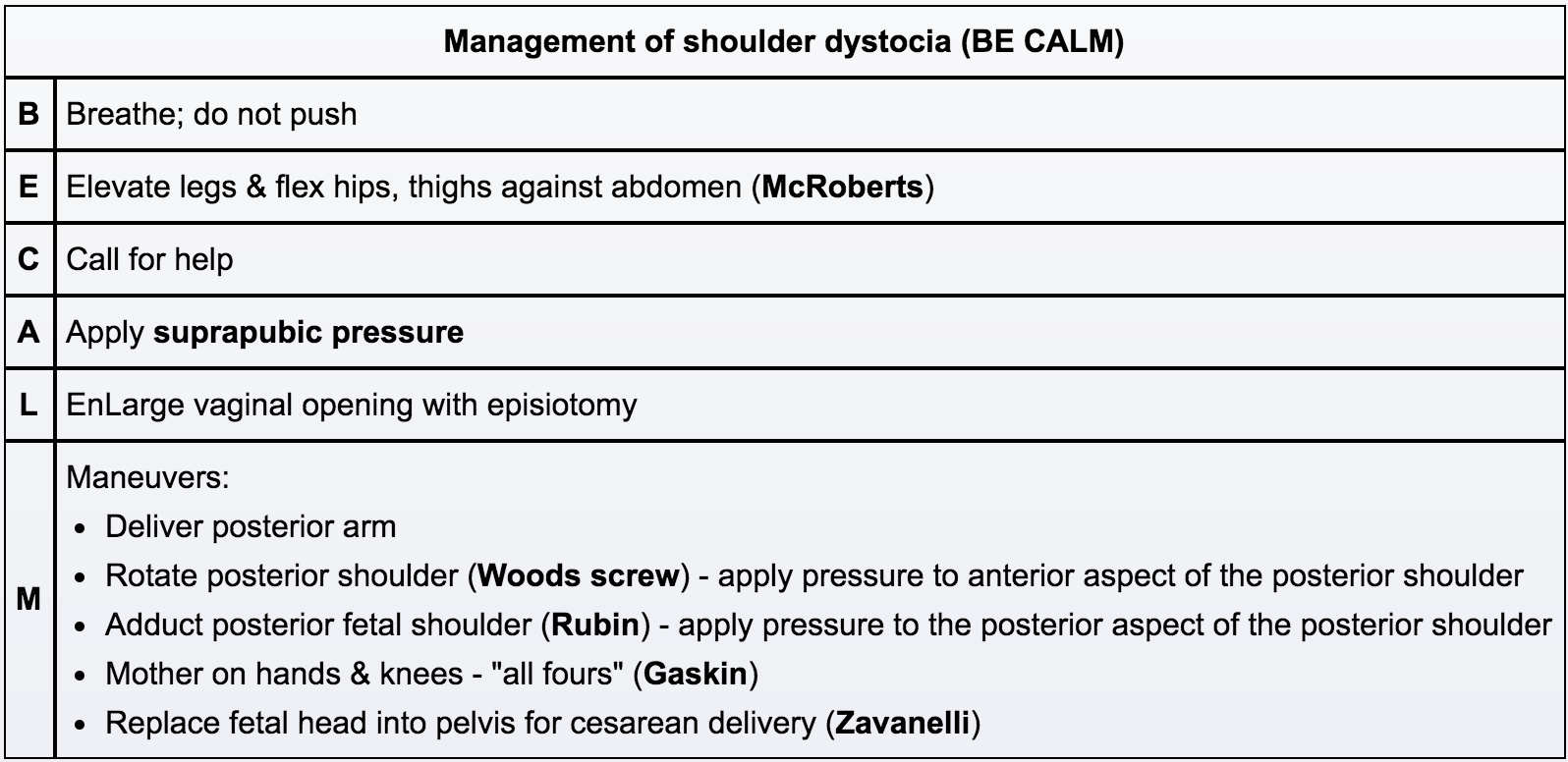
This algorithm is a fantastic way to remember the sequence of events. Notice how it moves from simple external maneuvers to more complex internal ones.
Since these topics are very high-yield for the UKMLA, would you like to try a quick quiz to see how well you can recall the management steps under pressure?
✍️ Obstetric Emergencies Quiz
Tap to practice questions in the Oncourse app
I've set up a 10-question quiz for you to test your knowledge on these emergencies. It's a great way to make sure those management steps are locked in!
Whenever you're ready, you can jump in and give it a go. Is there anything else about these emergencies you'd like to dive deeper into?
Setting up chat...