Medications in pregnancy: which drugs are safe, teratogenic and contraindicated
Prescribing in pregnancy is one of those high-stakes areas where you're always balancing the health of the mother with the potential risks to the developing fetus. It's a classic exam favorite because the "never-ever" drugs are so distinct!
Let me find a good visual to help you visualize the critical periods of fetal development and how drugs might interfere.
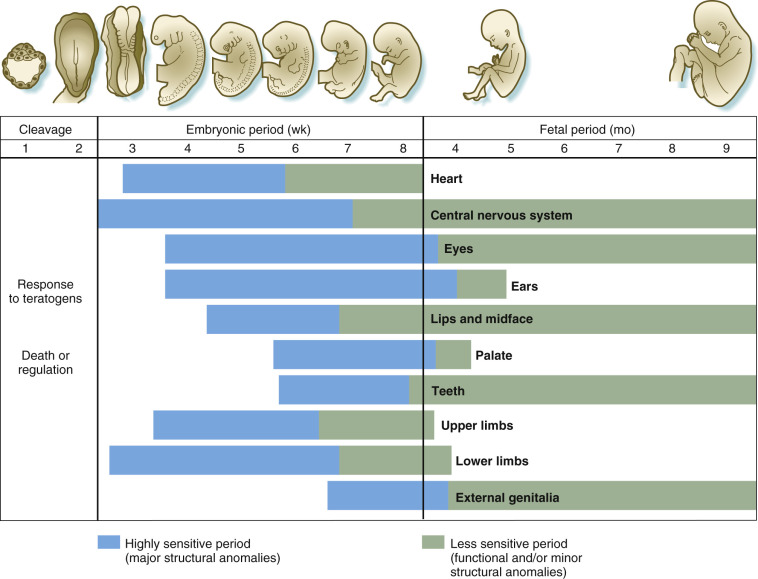
This diagram highlights that the embryonic period (weeks 3-8) is the most critical window for major structural malformations, while the fetal period is more associated with functional defects.
To make this easier to digest, I've put together a summary table of the most common drugs you'll encounter in exams and clinical practice, categorized by their safety profile.
| Drug Class | Safe / Preferred | Teratogenic / Contraindicated | Key Risks / Notes |
|---|---|---|---|
| Analgesics | Paracetamol | NSAIDs (esp. 3rd trimester) | NSAIDs: Premature closure of ductus arteriosus, oligohydramnios. |
| Antibiotics | Penicillins, Cephalosporins, Erythromycin | Tetracyclines, Aminoglycosides, Quinolones | Tetracyclines: Tooth discoloration, bone growth inhibition. Aminoglycosides: Ototoxicity. |
| Antihypertensives | Labetalol, Nifedipine, Methyldopa | ACE inhibitors, ARBs | ACEi/ARBs: Renal dysgenesis, skull defects, oligohydramnios. |
| Anticonvulsants | Levetiracetam, Lamotrigine (with high-dose folate) | Sodium Valproate, Phenytoin | Valproate: Neural tube defects (highest risk). Phenytoin: Fetal Hydantoin Syndrome. |
| Anticoagulants | LMWH (Heparin) | Warfarin | Warfarin: Fetal Warfarin Syndrome (bone/cartilage defects, CNS issues). |
| Antidiabetics | Insulin, Metformin | SGLT2 inhibitors | Insulin is the gold standard; Metformin is increasingly used. |
| Retinoids | None (Topical/Oral) | Isotretinoin | ABSOLUTE CONTRAINDICATION. Severe craniofacial, cardiac, and CNS defects. |
| Thyroid | Propylthiouracil (1st trim), Carbimazole (2nd/3rd) | Carbimazole (in 1st trim) | Carbimazole in 1st trimester: Aplasia cutis, choanal atresia. |
That table covers the heavy hitters you'll see on the UKMLA AKT. A few extra high-yield nuggets to keep in mind:
- Sodium Valproate: This is the "never" drug for women of childbearing age unless there's absolutely no alternative. It has the highest risk of neural tube defects and neurodevelopmental issues.
- Isotretinoin (Roaccutane): This is so teratogenic that patients must be on a Pregnancy Prevention Programme (PPP), including monthly pregnancy tests and dual contraception.
- ACE Inhibitors/ARBs: These are notorious for causing fetal renal dysgenesis and oligohydramnios (low amniotic fluid), which can lead to Potter's sequence.
- Warfarin: Unlike Heparin (which doesn't cross the placenta), Warfarin is a small molecule that crosses easily and causes Fetal Warfarin Syndrome (stippled epiphyses, nasal hypoplasia).
Let me pull up some lessons and flashcards so you can lock these in!
📚 Pregnancy Pharmacology Lessons
Those lessons on Medication safety in pregnancy and Teratogens and critical periods are perfect for your UKMLA prep.
To help you memorize the specific drug-risk pairings, let's pull up some flashcards.
🗂️ Pregnancy Medication Flashcards
Tap to study 30 flashcards in the Oncourse app
Those flashcards are a great way to test your recall on the fly.
One last thing to remember for your clinical rotations: always check the BNF (British National Formulary) or the UK Teratology Information Service (UKTIS) if you're ever unsure. Guidelines can change, and "safe" can sometimes be a relative term depending on the trimester!
Would you like to try a quick quiz to see how much of this stuck, or maybe a game of Synapses to group these drugs by their safety profile?
Setting up chat...