Major depressive disorder: DSM-5 criteria, antidepressant selection and side effects
Major Depressive Disorder (MDD) is a heavy hitter in psychiatry, and for the USMLE, you really need to know the diagnostic "math" and the side effect profiles of the meds we use to treat it. It’s not just about feeling sad; it’s a specific constellation of symptoms that persist for at least 2 weeks.
DSM-5 Diagnostic Criteria
To make the diagnosis, a patient must have 5 or more of the following symptoms for at least 2 weeks, and at least one of the symptoms must be either depressed mood or anhedonia (loss of interest/pleasure).
A classic way to remember these is the mnemonic SIGECAPS:
- Sleep: Insomnia or hypersomnia
- Interest: Anhedonia (this is a big one!)
- Guilt: Feelings of worthlessness or inappropriate guilt
- Energy: Fatigue or loss of energy
- Concentration: Diminished ability to think or indecisiveness
- Appetite: Weight loss or gain, or change in appetite
- Psychomotor: Agitation or retardation (must be observable by others)
- Suicidal ideation: Recurrent thoughts of death or suicide attempts
Antidepressant Selection & Side Effects
Choosing the right med usually starts with the "least-harm" principle. We typically start with SSRIs because they have a better safety profile compared to the older stuff.
I've put together a quick comparison of the major classes and the "red flag" side effects you'll likely see on your exam.
| Drug Class | Examples | Key Side Effects | Clinical Pearls |
|---|---|---|---|
| SSRIs | Fluoxetine, Sertraline, Escitalopram | Sexual dysfunction, GI upset, weight changes | First-line; takes 4-6 weeks for effect. |
| SNRIs | Venlafaxine, Duloxetine | Hypertension (Venlafaxine), sedation | Good for depression + chronic pain/fibromyalgia. |
| Atypical | Bupropion | Seizures (at high doses/bulimia), insomnia | No sexual side effects or weight gain! Avoid in eating disorders. |
| Atypical | Mirtazapine | Sedation, weight gain (increased appetite) | Great for elderly patients with insomnia/weight loss. |
| TCAs | Amitriptyline, Nortriptyline | The 3 C's: Coma, Convulsions, Cardiotoxicity (Arrhythmias) | Anticholinergic effects (dry mouth, urinary retention). |
| MAOIs | Phenelzine, Selegiline | Hypertensive crisis with tyramine (cheese/wine) | Risk of Serotonin Syndrome if combined with SSRIs. |
That table covers the high-yield side effects you'll likely see in clinical vignettes. For example, if a patient is worried about weight gain or sexual dysfunction, Bupropion is often the "correct" answer. If they're an elderly patient who can't sleep and has lost weight, Mirtazapine is your friend.
Let's look for a visual to help you visualize the diagnostic pathway or the neurotransmitter involvement.
This table is a goldmine for your differential diagnosis questions. It helps you distinguish between MDD, Adjustment Disorder, and a normal stress response—a very common USMLE trap!
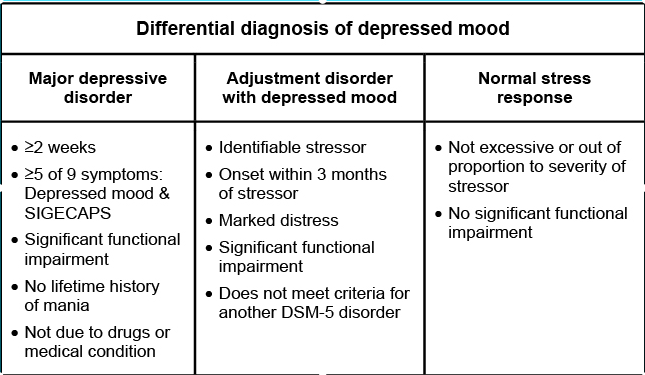
This chart highlights the key differences: MDD requires at least 5 SIGECAPS symptoms for 2+ weeks, while Adjustment Disorder is a reaction to a specific stressor within 3 months.
To really lock this in, let's pull up some detailed lessons and flashcards for your review.
📚 MDD & Antidepressants Lessons
Those lessons are great for a deep dive into the criteria and pharmacology. Now, let's get some flashcards to help you drill those side effects and diagnostic rules.
🗂️ MDD & Antidepressants Flashcards
Tap to study 13 flashcards in the Oncourse app
Those flashcards should help you nail the side effect profiles, especially the common ones like sexual dysfunction with SSRIs.
To wrap it up, remember the SIGECAPS mnemonic for the diagnosis and always look for those "deal-breaker" side effects in the vignettes when choosing an antidepressant. If you're feeling ready, I can set up a quick quiz for you to test your knowledge on these concepts!
Setting up chat...