Lung compliance and elastance: surfactant, fibrosis and emphysema effects
Lung compliance and elastance are two sides of the same coin when it comes to how our lungs handle air. Think of it like a rubber band: compliance is how easily you can stretch it out, while elastance is how quickly it snaps back to its original shape.
In the lungs:
- Compliance ($C = \Delta V / \Delta P$): The "distensibility" or ease with which the lungs expand.
- Elastance ($E = 1/C$): The "recoil" or the tendency of the lungs to return to their resting volume.
Let's look at how specific conditions and substances change this balance.
1. Surfactant: The Compliance Booster
Surfactant is a mix of lipids and proteins (mostly dipalmitoylphosphatidylcholine) produced by Type II pneumocytes. Its main job is to reduce surface tension at the air-liquid interface of the alveoli.
- Effect: By lowering surface tension, surfactant prevents small alveoli from collapsing (atelectasis) and increases lung compliance.
- Clinical Correlation: In Neonatal Respiratory Distress Syndrome (NRDS), a lack of surfactant leads to stiff, non-compliant lungs, making it incredibly hard for the infant to breathe.
2. Fibrosis: The Stiff Lung
In restrictive lung diseases like Idiopathic Pulmonary Fibrosis, the normal lung tissue is replaced by thick, scarred collagen.
- Effect: This makes the lungs very "stiff." Compliance decreases, and elastance increases (the lungs want to snap shut).
- Result: Patients have to work much harder to pull air in, leading to low lung volumes (decreased TLC, FRC, and RV).
3. Emphysema: The Floppy Lung
Emphysema (a type of COPD) involves the destruction of alveolar walls and elastic fibers, usually due to an imbalance between proteases (like elastase) and antiproteases (like $\alpha_1$-antitrypsin).
- Effect: With the loss of elastic tissue, the lungs lose their "snap-back." Compliance increases (they are very easy to fill), but elastance decreases.
- Result: While air gets in easily, the airways collapse during expiration, leading to air trapping and a "barrel chest" (increased TLC, FRC, and RV).
I'll pull up a table to help you compare these changes side-by-side, along with a diagram to visualize the pressure-volume loops.
| Feature | Compliance | Elastance | Pathophysiology |
|---|---|---|---|
| Normal + Surfactant | High | Normal | Surfactant reduces surface tension |
| Fibrosis | Low (Stiff) | High (Recoil) | Excess collagen/scarring |
| Emphysema | High (Floppy) | Low (No Recoil) | Destruction of elastic fibers |
I've summarized the key differences in the table above to help you keep them straight for your exams.
To help you visualize how these changes look on a pressure-volume curve, let me find a diagram that shows the shifts seen in fibrosis and emphysema.
The diagram below is a classic for USMLE prep. It shows how the pressure-volume curve shifts: left and steeper in emphysema (high compliance) and right and flatter in fibrosis (low compliance).
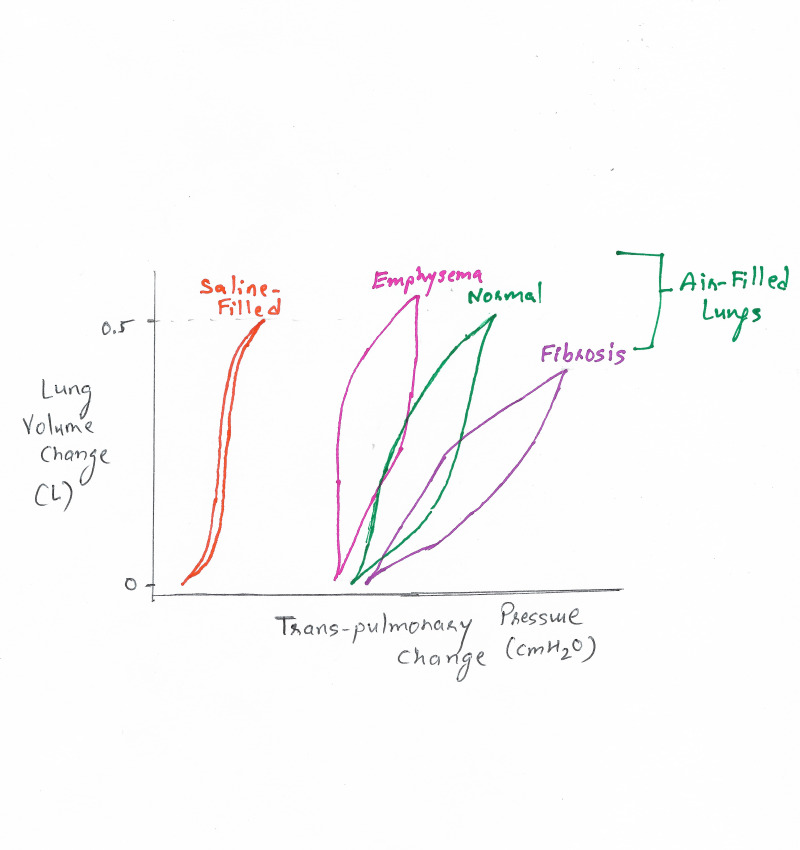
This graph illustrates how lung volume changes in response to transpulmonary pressure. Notice how the emphysema curve reaches higher volumes at lower pressures, while the fibrosis curve requires much higher pressure just to achieve a small change in volume.
To wrap this up, remember the "Rubber Band vs. Plastic Bag" analogy:
- Fibrosis is like a thick, heavy-duty rubber band (high elastance, low compliance).
- Emphysema is like an old, stretched-out plastic bag (low elastance, high compliance).
Would you like to try a few practice questions on this to see how it's tested, or should I find some flashcards for your review?
Setting up chat...