Diseases of the larynx: vocal cord paralysis, laryngeal tumors and hoarseness
That's a heavy-hitting trio of topics! The larynx is basically the "gatekeeper" of the airway and the "instrument" of our voice, so when things go wrong here, it's usually pretty high-stakes.
Since you're prepping for exams like NEET-PG or INI-CET, these topics are high-yield because they involve complex anatomy (hello, Recurrent Laryngeal Nerve!) and critical diagnostic dilemmas.
Let's start by looking at some key lessons to get the foundational theory down.
📚 Laryngeal Disease Lessons
Those lessons cover the core theory, but let's break down the clinical "meat" of these conditions.
1. Hoarseness (Dysphonia)
Hoarseness is a symptom, not a diagnosis. The most important rule for exams and clinical practice: Any patient with hoarseness for >3 weeks needs a direct or indirect laryngoscopy to rule out malignancy.
2. Vocal Cord Paralysis
This is all about the Recurrent Laryngeal Nerve (RLN).
- Unilateral RLN Palsy: The cord usually sits in the paramedian position. The voice is breathy/hoarse, but the airway is usually fine.
- Bilateral RLN Palsy: This is a medical emergency! Both cords are in the paramedian position, causing a narrow glottis. The voice might actually be okay, but the patient will have stridor and respiratory distress.
3. Laryngeal Tumors
- Benign: Vocal nodules (Singer's nodes - bilateral), Polyps (unilateral), and Papillomas (HPV 6, 11).
- Malignant: Squamous Cell Carcinoma is the king here.
- Glottic (Vocal cords): Presents early with hoarseness. Good prognosis because of sparse lymphatics (less spread).
- Supraglottic: Presents late (throat pain, dysphagia). Worse prognosis due to rich lymphatics.
To help you visualize the nerve supply—which is where most students get tripped up—let me find a good diagram of the laryngeal innervation.
That diagram is a classic for a reason! Notice how the Left Recurrent Laryngeal Nerve loops under the aortic arch—this is why a patient with a massive left atrium (Mitral Stenosis) or a lung tumor (Pancoast tumor) can present with hoarseness (Ortner's Syndrome).
Let's look at the visual representation of that anatomy.
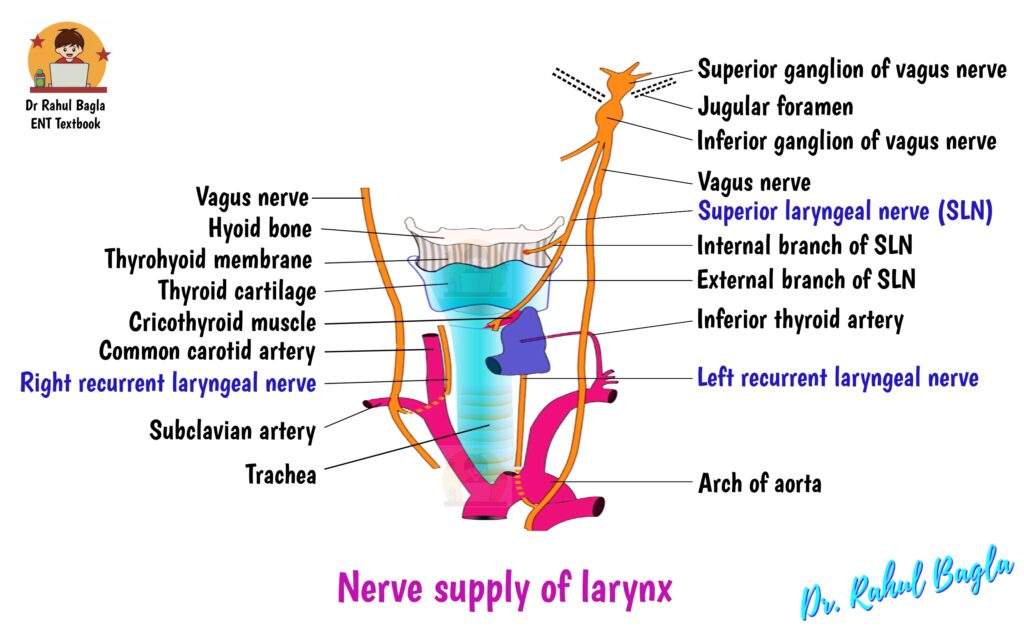
The diagram shows why the Left RLN is more commonly paralyzed than the right—it has a much longer course.
Now, let's talk about Laryngeal Cancer management. For early-stage (T1, T2) glottic cancer, both Radiotherapy and Transoral Laser Microsurgery are excellent options with high cure rates. For advanced stages (T3, T4), we're usually looking at Total Laryngectomy or Chemoradiation.
To help you differentiate between the various types of vocal cord positions in paralysis, I'll create a quick comparison table.
| Position | Nerve Involved | Voice Quality | Airway Status |
|---|---|---|---|
| Median | Normal | Normal | Normal |
| Paramedian | RLN Paralysis | Hoarse/Breathy | Usually Adequate |
| Cadaveric | RLN + SLN Paralysis | Very Breathy/Weak | Adequate |
| Bilateral Paramedian | Bilateral RLN | Good Voice | Stridor/Emergency |
That table is a lifesaver for those tricky ENT questions! Remember, the Cricothyroid muscle is the only one supplied by the External branch of the Superior Laryngeal Nerve (SLN). If that's intact, the cord stays in the paramedian position. If both RLN and SLN are gone, the cord drifts out to the Cadaveric position.
Since this is a high-yield topic for your PG exams, would you like to try a few practice questions to see how this translates into clinical scenarios?
✍️ Laryngeal Disease Quiz
Tap to practice questions in the Oncourse app
That quiz should give you a good idea of how these concepts are tested. Pay special attention to the management of bilateral RLN palsy—it's a classic "next best step" question (usually Tracheostomy or Lateralization of the cord).
If you're feeling a bit overwhelmed by the different types of laryngeal tumors, we could also try a quick Synapses game to group them by their characteristics. Or, if you're ready to move on, let me know!
Setting up chat...