Labor complications: shoulder dystocia, cord prolapse, postpartum hemorrhage
Oh, we're diving into the "big three" of obstetric emergencies! These are the scenarios that get every resident's heart racing, but having a solid game plan makes all the difference.
Let's break these down one by one so you're ready for any shelf exam or clinical rotation question that comes your way.
1. Shoulder Dystocia
This happens when the baby's head delivers, but the anterior shoulder gets stuck behind the mother's pubic symphysis. The classic sign is the "Turtle Sign" (the head retracts back against the perineum).
- Management (The ALARMER mnemonic):
- McRoberts Maneuver: Hyperflexing the mother's legs against her abdomen (this is usually the first step!).
- Suprapubic Pressure: Pushing down just above the pubic bone to dislodge the shoulder.
- Internal Maneuvers: Like the Woods' Screw or Rubin maneuver.
- Complications: Watch out for Erb-Duchenne palsy (C5-C6 injury, "waiter's tip" position) or clavicular fractures.
2. Umbilical Cord Prolapse
This is a true "run to the OR" emergency. The cord slips down into the vagina ahead of the baby, and the presenting part compresses it, cutting off oxygen.
- Key Finding: Sudden, severe variable decelerations or bradycardia on the fetal heart rate monitor after the membranes rupture.
- Immediate Action:
- Keep your hand in the vagina and manually elevate the fetal presenting part to take pressure off the cord.
- Place the mother in the Trendelenburg or knee-chest position.
- Emergency C-section is almost always the definitive move.
3. Postpartum Hemorrhage (PPH)
Defined as >500 mL loss after vaginal birth or >1000 mL after a C-section. The most common cause by far is Uterine Atony (the "boggy" uterus).
- The 4 T's of PPH:
- Tone: Uterine atony (most common).
- Tissue: Retained products of conception (placenta).
- Trauma: Lacerations or uterine rupture.
- Thrombin: Coagulopathy (like DIC).
I've got some great visual aids and practice materials to help lock these in. Let's start with a clear comparison of the management steps for these emergencies.
| Complication | Primary Risk Factor | Key Diagnostic Sign | First-Line Management |
|---|---|---|---|
| Shoulder Dystocia | Fetal Macrosomia (e.g., Gestational Diabetes) | "Turtle Sign" | McRoberts Maneuver & Suprapubic Pressure |
| Cord Prolapse | Malpresentation (Breech), Polyhydramnios | Sudden Variable Decelerations | Manually elevate presenting part; Emergency C-section |
| Postpartum Hemorrhage | Uterine Overdistension, Prolonged Labor | "Boggy" uterus (for Atony) | Uterine massage & Oxytocin |
Since these topics are high-yield for the USMLE and shelf exams, I'll pull up some specific lessons that go deeper into the maneuvers and medications used for each.
📚 Labor Complications Lessons
Those lessons will give you the full breakdown of the maneuvers and the specific drug dosages for PPH (like Oxytocin, Methylergonovine, and Carboprost).
To help you visualize the McRoberts maneuver and the "Turtle Sign," let me find a diagram for you.
The McRoberts maneuver is usually the first thing you'll do in a shoulder dystocia case because it's non-invasive and highly effective at opening up the pelvic outlet.
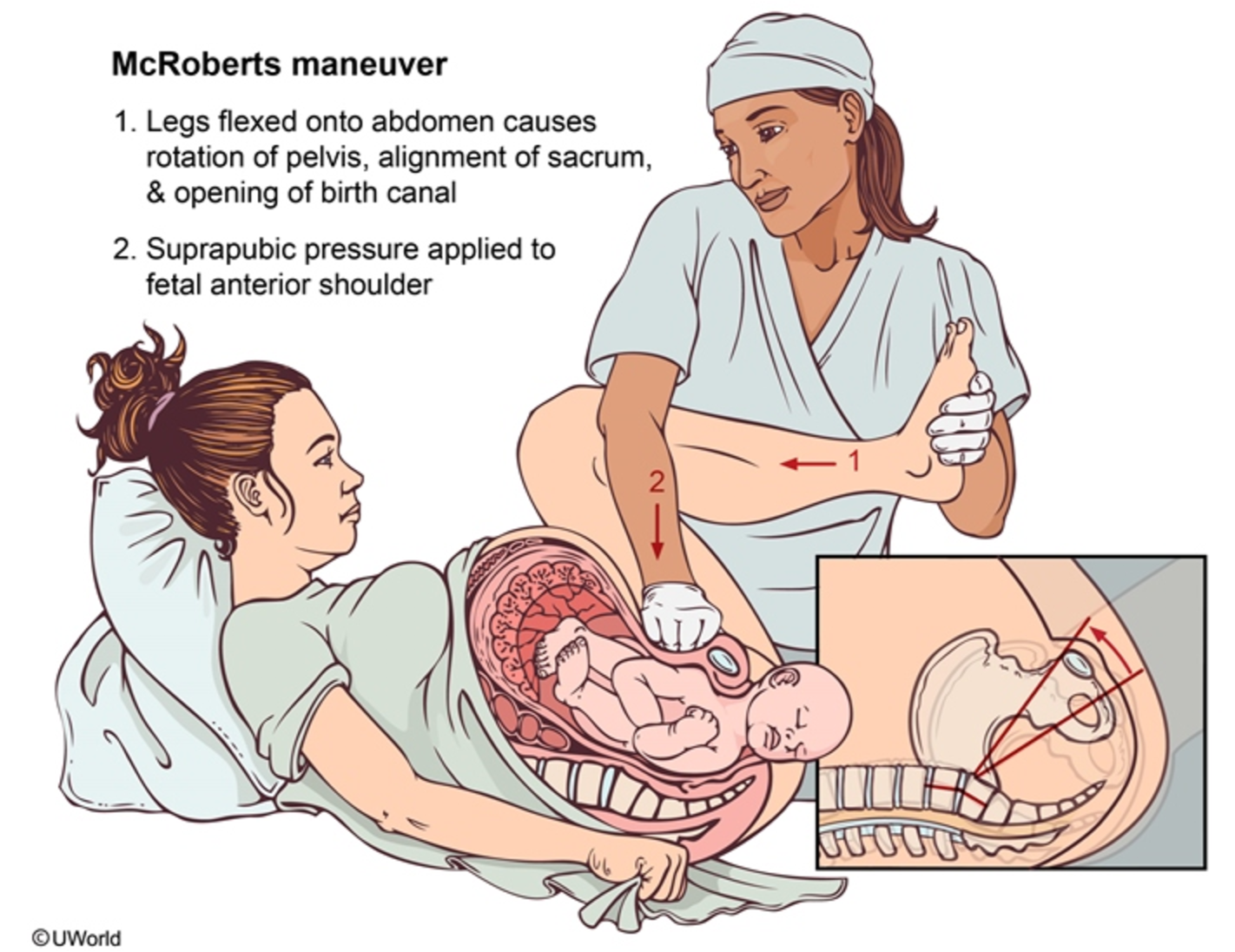
That diagram really shows how hyperflexing the hips helps rotate the pelvis to give that shoulder some room.
Since these are high-stakes topics, would you like to try a few practice questions to see how they're tested, or maybe some flashcards to memorize the drug contraindications for PPH? (For example, remember that Methylergonovine is contraindicated in hypertension, and Carboprost is a no-go for asthma!)
Setting up chat...