Knee injuries: ACL, meniscus tears, examination tests and management
Knee injuries are a classic high-yield topic for the AKT, especially since they often present in primary care or A&E. Let's break down the big ones: ACL ruptures and meniscus tears.
1. Anterior Cruciate Ligament (ACL) Injury
This usually happens during a "non-contact" twisting injury (like pivoting in football or skiing).
- Presentation: Patients often describe a loud "pop" followed by immediate, significant swelling (hemarthrosis within 0-2 hours) and a feeling of the knee "giving way."
- Examination Tests:
- Lachman Test: The most sensitive test. With the knee at 20-30° flexion, you pull the tibia forward. A "mushy" or absent end-point suggests a tear.
- Anterior Drawer Test: Similar to Lachman but with the knee at 90°. Less sensitive because the hamstrings can guard and stabilize the joint.
- Management:
- Initial: RICE (Rest, Ice, Compression, Elevation) and crutches.
- Long-term: Intense physiotherapy is first-line. Surgery (ACL reconstruction) is usually reserved for young, active individuals or those with persistent instability.
2. Meniscal Tears
These are often caused by a twisting injury while the foot is fixed, but the onset is usually more gradual than an ACL tear.
- Presentation: Pain is localized to the joint line. Swelling (effusion) often develops more slowly (over 6-24 hours). Key symptoms include locking (unable to fully extend the knee) or catching.
- Examination Tests:
- McMurray’s Test: Flex the knee and rotate the tibia while extending. A palpable "click" or pain at the joint line is positive.
- Thessaly Test: The patient stands on one leg (knee flexed to 20°) and twists. This is quite specific for meniscal pathology.
- Management:
- Small tears often settle with conservative management (physio).
- If the knee is "locked," it usually requires urgent orthopedic referral for arthroscopic repair or partial meniscectomy.
I'll pull up some high-yield lessons that cover these clinical features and the specific exam maneuvers you'll need to know for the UKMLA.
📚 Knee Injury Lessons
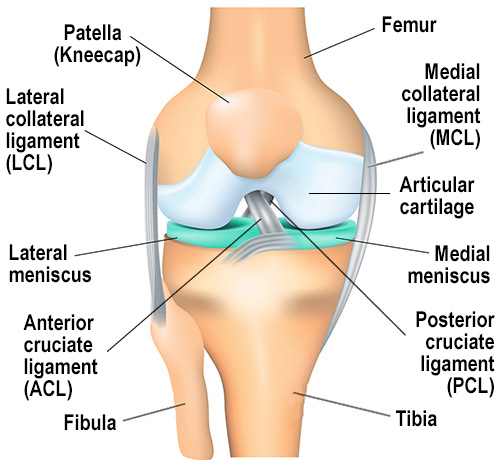
Visualizing the anatomy and the specific tests can really help things click. Let me find a diagram that shows the knee ligaments and the joint line, which is so important for diagnosing these.
Here is a clear look at the anatomy. Notice how the ACL sits deep in the center to prevent the tibia from sliding forward, while the menisci act as the shock-absorbing "cushions" on the joint line.
To help you differentiate these in a clinical scenario, here's a quick comparison table of the key features.
| Feature | ACL Rupture | Meniscal Tear |
|---|---|---|
| Mechanism | Non-contact twisting/pivoting | Twisting on a weight-bearing knee |
| Onset of Swelling | Rapid (within 0-2 hours) | Slower (6-24 hours) |
| Key Symptoms | "Pop" sound, instability ("giving way") | Joint line pain, locking, catching |
| Effusion Type | Hemarthrosis (blood) | Serous effusion (fluid) |
| Special Tests | Lachman, Anterior Drawer | McMurray, Thessaly |
| Management | Physio (conservative) or Reconstruction | Physio or Arthroscopic repair |
One last high-yield tip for the AKT: Ottawa Knee Rules. These help you decide if an X-ray is needed for an acute knee injury. You should order an X-ray if any of these are present:
- Age 55 or older
- Isolated tenderness of the patella
- Tenderness at the head of the fibula
- Inability to flex to 90°
- Inability to bear weight (4 steps) immediately and in the A&E department
Would you like to try a few practice questions on this to see how it's tested?
Setting up chat...