Infective endocarditis: Duke criteria, blood cultures and empirical antibiotics
Infective Endocarditis (IE) is one of those high-stakes topics that shows up in almost every UKMLA AKT paper. It’s essentially a "perfect storm" where bacteria (usually from the mouth, skin, or gut) find their way onto the heart valves, leading to vegetation and systemic chaos.
Let's break this down into the three pillars you asked about: the diagnostic criteria, the culture protocol, and the initial treatment.
1. The Modified Duke Criteria
To make a definitive diagnosis of IE, we use the Modified Duke Criteria. It’s a bit of a "mix and match" system based on Major and Minor criteria.
Definite IE is diagnosed if you have:
- 2 Major criteria
- 1 Major + 3 Minor criteria
- 5 Minor criteria
I've put together a table to help you distinguish between the two categories:
| Category | Criteria Details |
|---|---|
| Major Criteria | 1. Positive Blood Cultures: Typical organism from 2 separate cultures OR persistently positive cultures. 2. Endocardial Involvement: Positive Echo (vegetation, abscess, new valvular regurgitation) OR new murmur. |
| Minor Criteria | 1. Predisposition: IV drug use or pre-existing heart condition. 2. Fever: Temp > 38°C. 3. Vascular Phenomena: Emboli, Janeway lesions, mycotic aneurysm. 4. Immunological Phenomena: Glomerulonephritis, Osler's nodes, Roth spots, Rheumatoid Factor. 5. Microbiological Evidence: Positive culture that doesn't meet Major criteria. |
2. Blood Culture Protocol
In the UK, the protocol for blood cultures in suspected IE is very specific to ensure we catch the causative organism before antibiotics mask it.
- The "3 Sets" Rule: You must take 3 sets of blood cultures from separate peripheral sites.
- Timing: There should be at least 6 hours between the first and last set.
- Volume: Ensure adequate volume (usually 10ml per bottle) as the bacterial load can be low.
- Crucial Point: Always take cultures before starting empirical antibiotics unless the patient is in septic shock.
3. Empirical Antibiotics (UK Guidelines)
While we wait for those cultures to grow, we start empirical treatment based on whether the patient has a native valve or a prosthetic valve.
- Native Valve: Usually Amoxicillin (often with Gentamicin) OR Benzylpenicillin + Gentamicin. If the patient is penicillin-allergic or MRSA is suspected, Vancomycin + Gentamicin is the go-to.
- Prosthetic Valve: This is much harder to treat. The standard triple therapy is Vancomycin + Gentamicin + Rifampicin.
To help you visualize the classic physical signs mentioned in the Minor criteria (like those Osler's nodes and Janeway lesions), let me find a diagram for you.
These physical signs are classic "exam fodder" for the UKMLA. Remember that Osler's nodes are Ouchy (painful), while Janeway lesions are Just there (painless).
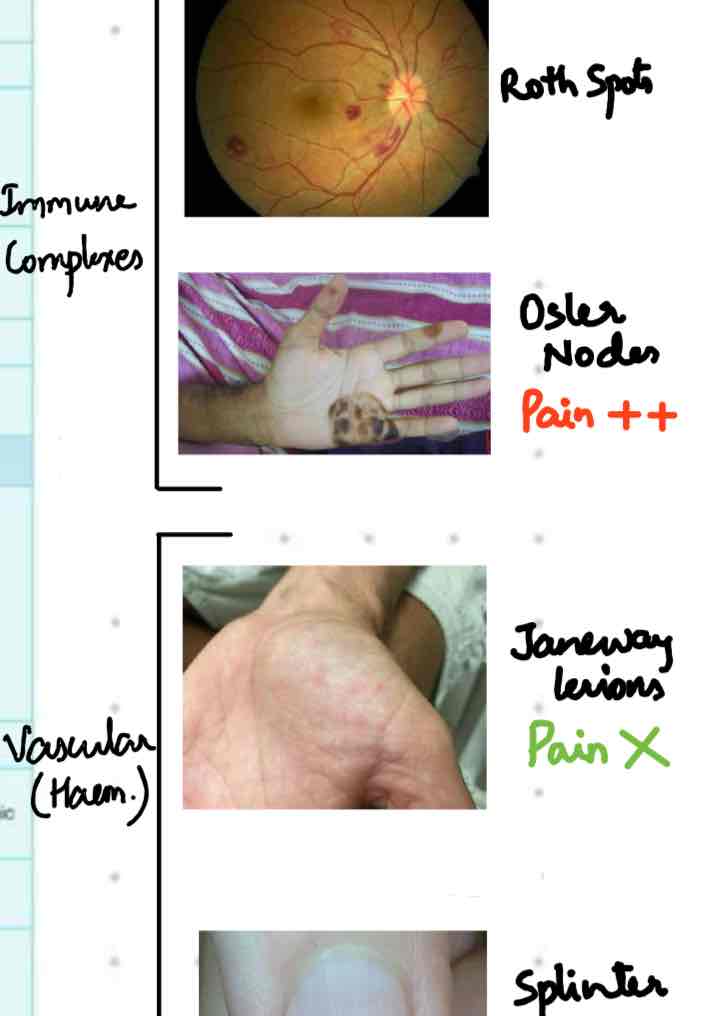
This image shows the classic "immunological" and "vascular" phenomena:
- Roth spots: Retinal hemorrhages with pale centers.
- Osler nodes: Painful, raised nodules on the pads of fingers/toes.
- Janeway lesions: Painless, flat macules on the palms/soles.
- Splinter hemorrhages: Linear streaks under the nails.
To help you lock this in for your AKT prep, I'll pull up some relevant lessons and flashcards for you to review.
Those lessons cover the pathology and management in detail. Let's also get some flashcards to help you memorize the Duke criteria and antibiotic regimens.
Those flashcards should help you drill the key points. One last high-yield tip for the AKT: if a patient has Streptococcus bovis (now often called S. gallolyticus) endocarditis, you must investigate for colorectal cancer. It's a classic association that examiners love!
Is there anything else about IE you'd like to dive into, or are you ready to test yourself with a quick quiz?
Setting up chat...