Irritable bowel syndrome: Rome IV criteria, red flags and NICE management
Ah, Irritable Bowel Syndrome (IBS)! It's a classic UKMLA topic because it's so common in primary care and requires a really structured approach to diagnosis and management. Since you're prepping for the AKT, focusing on the NICE guidelines and the Rome IV criteria is exactly where you want to be.
Rome IV Diagnostic Criteria
To diagnose IBS, a patient must have had recurrent abdominal pain, on average, at least 1 day per week in the last 3 months, associated with two or more of the following:
- Related to defecation (either increasing or improving pain).
- Associated with a change in frequency of stool.
- Associated with a change in form (appearance) of stool.
Note: Symptoms should have started at least 6 months before the diagnosis can be made.
The "Red Flags" (When it's NOT just IBS)
Before you slap an IBS label on someone, you have to rule out the scary stuff (Malignancy, IBD, Celiac). NICE is very specific about these:
- Unintentional weight loss
- Rectal bleeding
- Family history of bowel or ovarian cancer
- Onset of symptoms > 50 years old
- Anaemia (specifically iron-deficiency)
- Abdominal or rectal masses
- Raised inflammatory markers (CRP/ESR or Faecal Calprotectin)
NICE Management Strategy
NICE takes a stepped approach, starting with lifestyle and moving to targeted meds based on the predominant symptom (IBS-C, IBS-D, or IBS-M).
1. First-line Lifestyle & Diet:
- Regular meals and adequate fluid intake.
- Limit fresh fruit to 3 portions a day.
- High-fibre diet? Be careful—NICE suggests adjusting fibre intake (specifically avoiding insoluble fibre like bran) and trying ispaghula husk (soluble fibre) if needed.
- Probiotics: Try them for at least 4 weeks to see if they help.
2. Pharmacological (Symptom-based):
- Pain/Cramping: Antispasmodics (e.g., Mebeverine, Buscopan).
- Constipation: Laxatives (but avoid lactulose as it causes bloating!). Linaclotide is an option if others fail.
- Diarrhoea: Loperamide is the first-line choice.
3. Second-line (The "Psych" Meds):
- If first-line meds don't work after 12 months, NICE recommends low-dose Tricyclic Antidepressants (TCAs) like Amitriptyline (starting at 5-10mg). They act as visceral analgesics here, not just for mood!
I've put together a quick summary table of the management steps to help you visualize the "NICE way" of doing things.
[tool call: show_markdown_to_user] [tool call: assetSearch] [tool call: get_related_lessons_by_search_query]
Wait, I need to do them one by one.
Step 1: Show the table.I've put together a quick summary table of the management steps to help you visualize the "NICE way" of doing things.
| Symptom | First-line Management | Second-line / Specialist |
|---|---|---|
| Pain & Bloating | Antispasmodics (Mebeverine, Alverine, Peppermint oil) | Low-dose TCAs (e.g., Amitriptyline) |
| Constipation (IBS-C) | Soluble fibre (Ispaghula), Osmotic laxatives (Macrogol) | Linaclotide (if laxatives fail for 12+ months) |
| Diarrhoea (IBS-D) | Loperamide | Eluxadoline (Specialist use only) |
| Refractory | Dietitian referral (Low FODMAP diet) | Psychological therapies (CBT, Hypnotherapy) |
High-Yield Tip: Always check Faecal Calprotectin and Celiac Serology (IgA tTG) in primary care to rule out IBD and Celiac disease before confirming IBS!
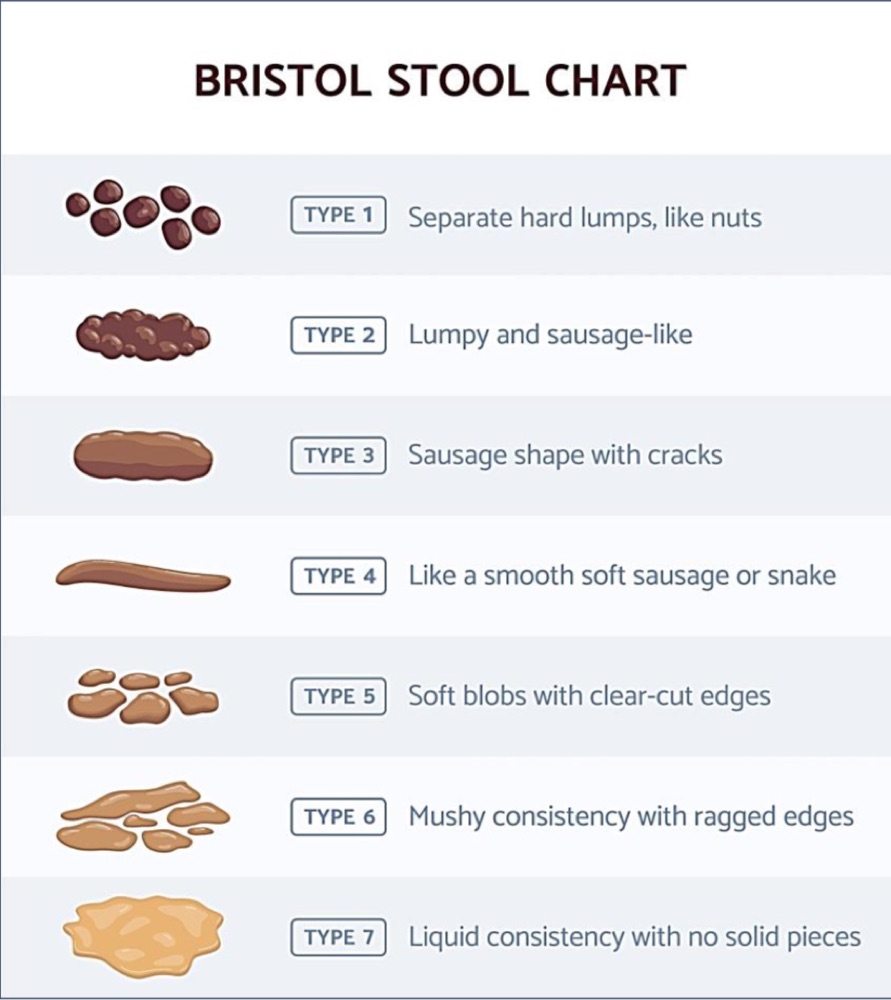
That table covers the essentials for the AKT. To help you visualize the different types of IBS, let's look at the Bristol Stool Chart—it's how we actually categorize IBS-C (Types 1-2) vs IBS-D (Types 6-7) in clinical practice.
The Bristol Stool Chart is a key tool for diagnosing IBS subtypes. For example, IBS-C is defined as having more than 25% of stools as Type 1 or 2, while IBS-D is more than 25% as Type 6 or 7.
To round this off, I've pulled up some high-yield lessons on IBS and its differentials like Celiac disease and IBD, which are essential for your AKT prep.
📚 IBS and Differentials Lessons
I hope that helps you nail those IBS questions! Remember, the key for the AKT is knowing when to stop diagnosing IBS and start investigating for something more serious. Let me know if you want to dive deeper into any of those differentials or try some practice questions!
Setting up chat...