HIV: testing, CD4 thresholds, ART initiation and opportunistic infections
HIV is a massive topic for the UKMLA AKT, but it's actually quite logical once you break it down into the "when to test," "when to treat," and "what to watch out for" categories. Since you're prepping for the UK exams, we'll stick closely to the British HIV Association (BHIVA) and NICE guidelines.
1. HIV Testing
In the UK, the standard screening test is the 4th generation ELISA, which looks for both the HIV-1/2 antibodies and the p24 antigen.
- Window Period: The p24 antigen can often be detected within 2-4 weeks, but for a definitive "all clear," testing is usually recommended at 4 weeks (for 4th gen tests) or 90 days for older tests.
- Who to test: Anyone with an indicator condition (like unexplained weight loss, chronic diarrhea, or certain skin conditions), all patients at GUM/antenatal clinics, and anyone in high-prevalence areas (where diagnosed prevalence is >2/1000) admitted to the hospital.
2. ART Initiation
The rule nowadays is simple: Treat everyone.
- BHIVA Guidelines: ART should be offered to all patients diagnosed with HIV, regardless of their CD4 count.
- Goal: To achieve an undetectable viral load (usually <50 copies/mL), which prevents transmission (U=U: Undetectable = Untransmittable) and preserves immune function.
I'll pull up some high-yield lessons on HIV management and the specific drug classes used in ART to help you dive deeper.
📚 HIV Management Lessons
The CD4 count is your best indicator of the patient's current immune status and their risk for specific opportunistic infections (OIs). A normal CD4 count is typically between 500-1500 cells/mm³.
As the CD4 count drops, the "gates" open for different pathogens. For the AKT, you absolutely need to know the thresholds for prophylaxis.
I've put together a summary table of the most common OIs and their corresponding CD4 thresholds to help you keep them straight.
| CD4 Count | Opportunistic Infection | Prophylaxis / Key Features |
|---|---|---|
| < 500 | Oral Thrush, Kaposi Sarcoma, TB | TB can occur at any CD4, but risk increases as it drops. |
| < 200 | Pneumocystis jirovecii (PCP) | Co-trimoxazole prophylaxis. Look for exertional desaturation. |
| < 100 | Toxoplasmosis, Cryptococcosis | Toxoplasmosis: Ring-enhancing lesions on CT. |
| < 50 | Mycobacterium avium complex (MAC), CMV | CMV: Retinitis (pizza-pie appearance) or colitis. |
It's also super helpful to visualize how the HIV virus actually works and where the different ART drug classes (like NRTIs, NNRTIs, and Protease Inhibitors) act. This is a common question on the AKT.
Let me find a diagram of the HIV life cycle for you.
This diagram is perfect for visualizing the HIV life cycle and where our ART drugs (like NRTIs, NNRTIs, and Protease Inhibitors) actually step in to stop the virus.
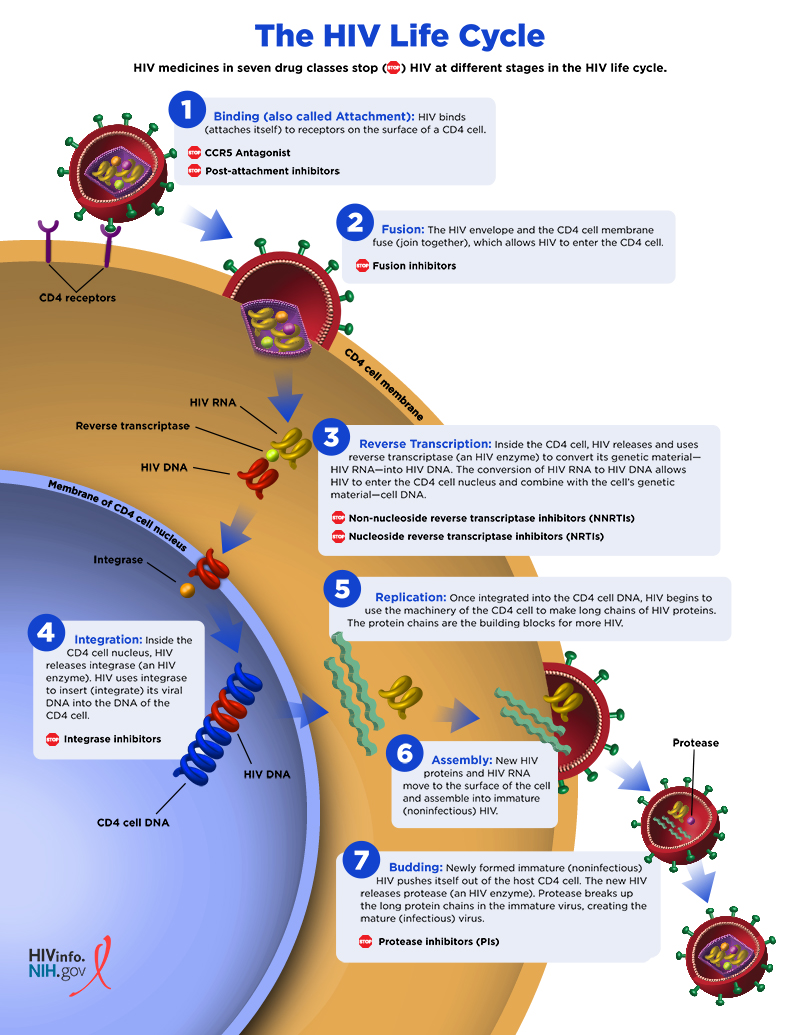
This diagram illustrates the seven stages of the HIV life cycle within a CD4 T cell and the corresponding antiretroviral (ART) drug intervention points, from viral binding to maturation.
To really lock this in for your AKT, would you like to try some flashcards on HIV testing and OIs?
🗂️ HIV Flashcards for AKT
Tap to study 10 flashcards in the Oncourse app
Those flashcards are a great way to drill the numbers. For the AKT, just remember the big three: test everyone (especially with indicator conditions), treat everyone (regardless of CD4), and prophylax for PCP if the CD4 count is below 200.
If you're feeling confident, we could jump into a quick quiz to see how these concepts show up in clinical scenarios. Ready to give it a go?
✍️ HIV & OIs Quiz for AKT
Tap to practice questions in the Oncourse app
Good luck with that quiz! It's a great way to see how these guidelines translate into clinical decisions. If any of the answers trip you up, or if you want to dive deeper into a specific opportunistic infection like PCP or Toxoplasmosis, just let me know. I'm here to help!
Setting up chat...