Hearing loss: types, audiometry interpretation and management
Hearing loss is one of those topics that shows up everywhere—from ENT clinics to high-yield PG entrance questions. It's basically divided into three main flavors based on where the "break" in the system is.
Types of Hearing Loss
- Conductive Hearing Loss (CHL): This happens when sound can't get through the outer or middle ear. Think of it as a mechanical issue—like a wax plug, a perforated eardrum, or fluid in the middle ear (serous otitis media).
- Sensorineural Hearing Loss (SNHL): This is "nerve deafness." The problem lies in the inner ear (cochlea) or the auditory nerve (CN VIII). Common causes include aging (presbycusis), loud noise exposure, or Ménière's disease.
- Mixed Hearing Loss: A bit of both! You'll see this in conditions like advanced otosclerosis or chronic suppurative otitis media (CSOM).
To help you visualize how we distinguish these on a graph, let me find a clear diagram of audiometry patterns for you.
That diagram perfectly illustrates the "Air-Bone Gap," which is the secret sauce for audiometry interpretation.
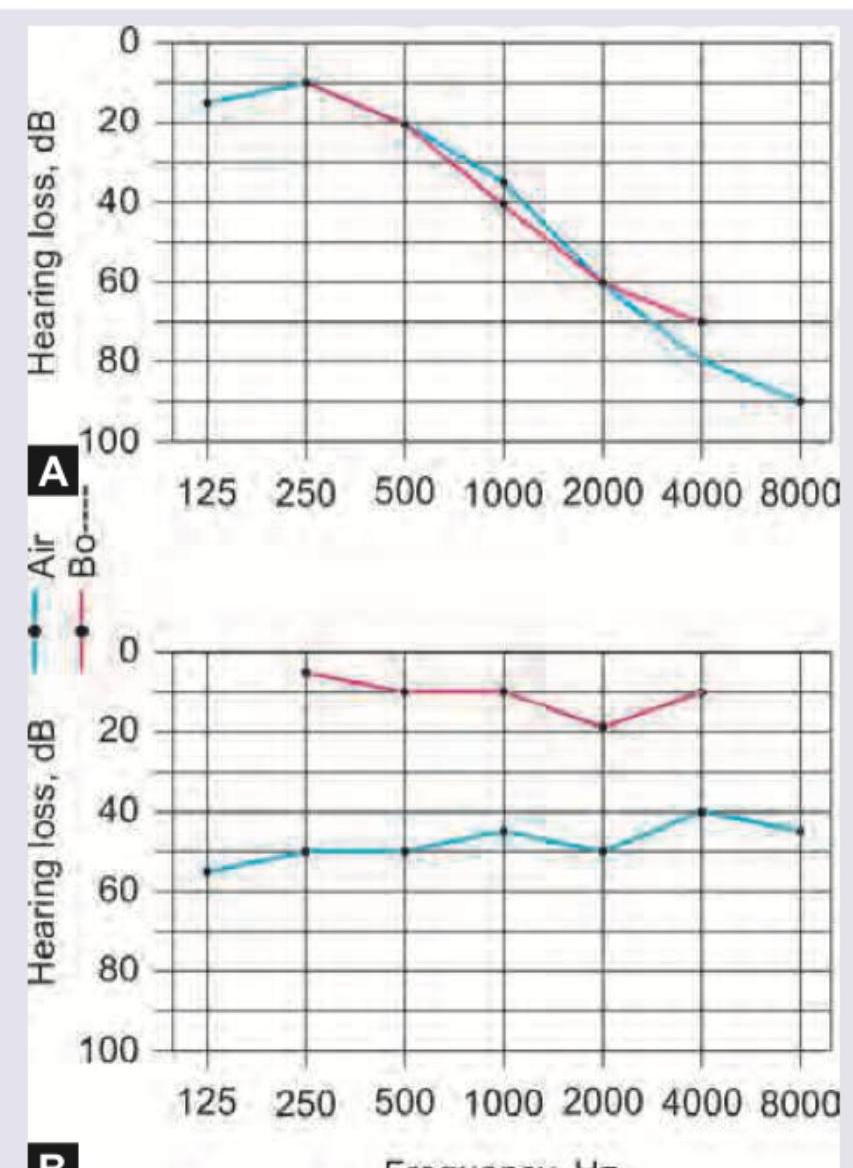
When you're looking at an audiogram, remember: Air Conduction (AC) tells you the total hearing, while Bone Conduction (BC) tells you the reserve (the health of the inner ear).
Audiometry Interpretation Rules
- Normal Hearing: Both AC and BC thresholds are between
0-25 dB. - Conductive (CHL): BC is normal, but AC is depressed. This creates an ==Air-Bone Gap > 15 dB==.
- Sensorineural (SNHL): Both AC and BC are depressed to the same level (No Air-Bone Gap).
- Mixed: Both are depressed, but AC is worse than BC (Air-Bone Gap is present).
Let's summarize the key differences and management strategies in a quick-reference table.
| Feature | Conductive Hearing Loss (CHL) | Sensorineural Hearing Loss (SNHL) |
|---|---|---|
| Site of Lesion | External or Middle Ear | Inner Ear (Cochlea) or VIII Nerve |
| Rinne Test | Negative (BC > AC) | Positive (AC > BC) |
| Weber Test | Lateralizes to the Poorer ear | Lateralizes to the Better ear |
| Audiometry | BC normal, AC depressed (AB Gap > 15dB) | Both AC & BC depressed (No AB Gap) |
| Management | Often treatable (Medical/Surgical) | Often permanent (Hearing Aids/Implants) |
| Common Causes | Wax, Otosclerosis, CSOM, ASOM | Presbycusis, Noise, Ototoxicity, Ménière's |
The management of hearing loss is all about the "why." If it's a mechanical blockage (CHL), we can often fix it with surgery or medicine. If it's a nerve issue (SNHL), we focus on amplification or bypassing the damaged part of the ear.
Management Strategies
- Conductive Hearing Loss:
- Medical: Antibiotics for infections (AOM/CSOM).
- Surgical: Myringotomy (for fluid), Stapedectomy (for otosclerosis), or Tympanoplasty (for perforated eardrums).
- Sensorineural Hearing Loss:
- Hearing Aids: The first line for mild to moderate SNHL.
- Cochlear Implants: For severe to profound bilateral SNHL where hearing aids aren't enough.
- Auditory Brainstem Implants (ABI): Used when the auditory nerve itself is damaged or absent (e.g., NF2).
To help you master this for your exams, I've pulled up some high-yield lessons and flashcards for you.
📚 Hearing Loss Lessons
Those lessons cover the high-yield topics like Sudden SNHL and Chronic Otitis Media (CSOM), which are classic exam favorites.
Let's also get some flashcards to lock in those audiometry patterns and management steps.
🗂️ Hearing Loss Flashcards
Tap to study 9 flashcards in the Oncourse app
Those flashcards are great for drilling the tuning fork tests and management of sudden SNHL.
Since you've got the theory down, would you like to try a quick game of Synapses to see if you can group these hearing loss causes and tests correctly? It's a fun way to make sure you don't mix them up in the exam!
Setting up chat...