Headache: migraine vs tension vs cluster — diagnosis and acute treatment
Headaches are a total bread-and-butter topic for the AKT, but keeping the "big three" straight can be tricky when you're under pressure. Let's start with a visual of where these usually hit, as the distribution is often your first big clue.
Seeing the distribution really helps differentiate them at a glance. Here's a classic diagram showing the typical patterns for tension and migraine.
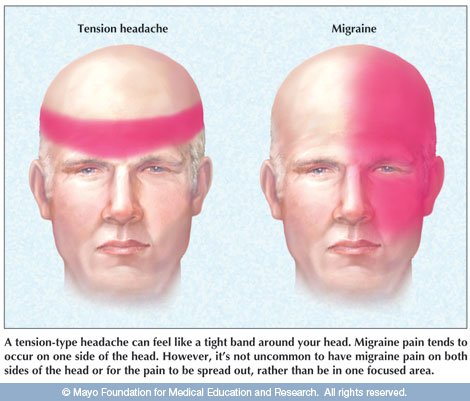
Note: Tension headaches are typically bilateral and "band-like," while migraines are often unilateral and throbbing.
To make things even clearer for your revision, I've put together a comparison table that includes Cluster headaches, which are the "alarm clock" headaches you definitely don't want to miss.
| Feature | Tension-Type (TTH) | Migraine | Cluster Headache |
|---|---|---|---|
| Pain Nature | Tight, "band-like," pressure | Pulsating, throbbing | Sharp, stabbing, "boring" |
| Location | Bilateral | Unilateral (usually) | Unilateral (periorbital/temporal) |
| Duration | 30 mins to 7 days | 4 to 72 hours | 15 to 180 mins |
| Frequency | Variable | Episodic | "Bouts" (1-8/day for weeks) |
| Associated Symptoms | None (usually) | Nausea, photo/phonophobia, aura | Autonomic (tearing, redness, ptosis, rhinorrhoea) |
| Activity Effect | Not aggravated by activity | Aggravated by activity (patient wants to lie in dark room) | Patient is restless, "pacing" the room |
| Acute Treatment | Aspirin, Paracetamol, NSAIDs | Oral Triptan + NSAID (or Paracetamol) | 100% Oxygen (12-15L) and/or SC/Nasal Triptan |
That table covers the essentials, but here are a few high-yield "pro-tips" for the AKT:
- Migraine Acute Management: NICE actually recommends combination therapy as first-line (an oral triptan PLUS an NSAID or Paracetamol). Also, consider an anti-emetic (like Metoclopramide) even if they aren't nauseated, as it helps with the gastric stasis that happens during a migraine.
- Cluster Headache "Must-Knows": The oxygen must be 100% high-flow (12-15L/min) via a non-rebreathe mask. Oral triptans are useless here because they take too long to kick in—you need subcutaneous or nasal Sumatriptan.
- Medication Overuse Headache: If a patient is using simple analgesics for $\ge$ 15 days/month or triptans/opioids for $\ge$ 10 days/month, suspect this! The treatment is (ironically) stopping the meds abruptly.
If you want to dive deeper into the prophylaxis or the specific "red flags" for secondary headaches (like SNOOP), I've pulled up some great lessons for you.
📚 Headache Management Lessons
Those lessons on red flags are particularly important for the AKT, as they often test your ability to spot when a headache isn't just a primary headache (like a subarachnoid hemorrhage or temporal arteritis).
Let me know if you want to practice some clinical cases or if you'd like to see the prophylaxis guidelines next!
Setting up chat...