GI pathology: inflammatory bowel disease, celiac, colorectal cancer
GI pathology is a massive topic, but it's also incredibly high-yield for the USMLE. Since you've mentioned Inflammatory Bowel Disease (IBD), Celiac disease, and Colorectal Cancer (CRC), we're looking at the "big hitters" of the gut.
I'll start by pulling up some comprehensive lessons on these topics so you have the full deep-dive available.
📚 GI Pathology Lessons
Those lessons will give you the granular details, but for the USMLE, the examiners love to make you distinguish between Crohn's and Ulcerative Colitis (UC).
I've put together a comparison table to help you keep the key differences straight—especially the "skip lesions" vs. "continuous involvement" and the depth of the inflammation.
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Location | Any part of GI tract (mouth to anus); Terminal ileum most common. | Colon only; always involves the rectum. |
| Pattern | Skip lesions (discontinuous). | Continuous involvement. |
| Depth | Transmural (all layers) -> leads to fistulas/strictures. | Mucosal and submucosal only. |
| Gross Findings | Cobblestone mucosa, creeping fat, string sign on X-ray. | Friable mucosa, pseudopolyps, lead pipe appearance (loss of haustra). |
| Microscopy | Non-caseating granulomas, Th1 mediated. | Crypt abscesses and ulcers, Th2 mediated. |
| Complications | Fistulas, strictures, malabsorption. | Toxic megacolon, higher risk of CRC, PSC. |
| Smoking | Smoking increases risk. | Smoking decreases risk (weird, right?). |
Now, let's talk Celiac Disease. The key for your exams is the association with HLA-DQ2/DQ8 and the specific pathology in the duodenum.
When you see a biopsy, you're looking for villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis. It's basically the gut's reaction to gluten (specifically gliadin).
I'll find a diagram of the duodenal changes so you can visualize that villous blunting.
The biopsy image below shows exactly what happens in Celiac disease: the normally tall, finger-like villi become flattened (atrophy), and the crypts (the "valleys" between villi) get deeper (hyperplasia).
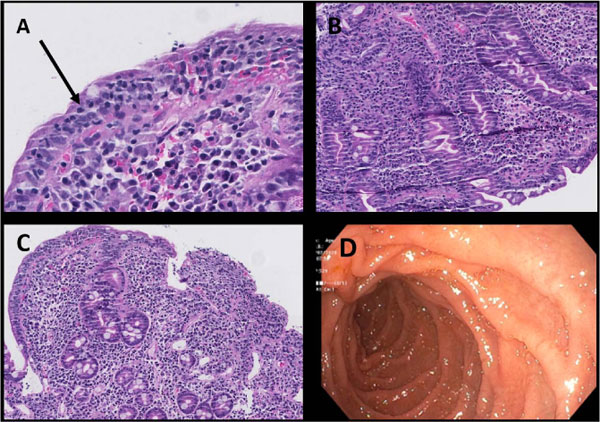
Notice the severe villous blunting and the dense inflammatory infiltrate in the lamina propria—this is why patients can't absorb nutrients properly.
Finally, for Colorectal Cancer (CRC), the USMLE loves the Adenoma-to-Carcinoma Pathway. It's a sequence of mutations:
- APC (loss of tumor suppressor) -> "At risk" epithelium
- KRAS (gain of oncogene) -> Adenoma formation
- p53 (loss of tumor suppressor) -> Carcinoma
I'll create a quick flowchart for this pathway so you can memorize the order of the mutations—it's a classic exam question.
The sequence of mutations in CRC is a classic "hit-by-hit" progression. One thing to remember: Aspirin and NSAIDs can actually reduce the risk of CRC because they inhibit COX-2, which is overexpressed in many adenocarcinomas.
I've covered the big three GI pathology topics for you. If you're feeling ready, I can pull up some practice questions to see how well you can distinguish these in a clinical scenario!
Setting up chat...