Gestational diabetes: screening, management and delivery timing
Gestational Diabetes Mellitus (GDM) is a super important topic for the UKMLA AKT, especially since the NICE guidelines are very specific about how we handle these pregnancies. It's essentially any degree of glucose intolerance with its onset or first recognition during pregnancy.
Let's break this down into the three areas you asked about: screening, management, and delivery.
1. Screening: The "Who" and "When"
In the UK, we don't screen everyone universally with a blood test; instead, we use risk factors.
Risk Factors for GDM:
- BMI > 30 kg/m²
- Previous macrosomic baby (≥ 4.5kg)
- Previous gestational diabetes
- First-degree relative with diabetes
- Minority ethnic origin with a high prevalence of diabetes
The Screening Process:
- If they've had GDM before: Offer early self-monitoring or an Oral Glucose Tolerance Test (OGTT) as soon as possible after booking, and another at 24–28 weeks if the first was normal.
- Other risk factors: Offer an OGTT at 24–28 weeks.
NICE Diagnostic Thresholds (OGTT):
- Fasting plasma glucose:
≥ 5.6 mmol/L- 2-hour plasma glucose:
≥ 7.8 mmol/L
2. Management: Step-by-Step
The goal is to keep blood glucose levels within a tight range to prevent complications like macrosomia or neonatal hypoglycemia.
- First Line: Diet and exercise. If targets aren't met within 1–2 weeks, move to medication.
- Metformin: Usually the first oral medication offered.
- Insulin: Started immediately if the fasting glucose is
> 7.0 mmol/Lat diagnosis, or if it's between6.0-6.9 mmol/Lwith complications like macrosomia or polyhydramnios.
3. Delivery Timing
We don't usually let these pregnancies go past their due date because of the risk of stillbirth and birth trauma.
- Well-controlled GDM: Offer elective birth (induction or C-section) between 37+0 and 40+6 weeks.
- Complicated GDM: If there are fetal or maternal complications, delivery is often earlier.
I'll pull up some high-yield lessons and a flowchart to help you visualize the management pathway, as that's usually where the tricky exam questions hide!
I've found a helpful flowchart that outlines the diagnostic and management pathway for GDM. While the specific glucose values in some diagrams can vary slightly by region (always stick to the NICE values of 5.6 fasting and 7.8 at 2 hours for the UK!), the logic of moving from lifestyle to medication remains the same.
GDM Management Pathway
I'll display this flowchart for you now to help visualize the progression from screening to treatment.
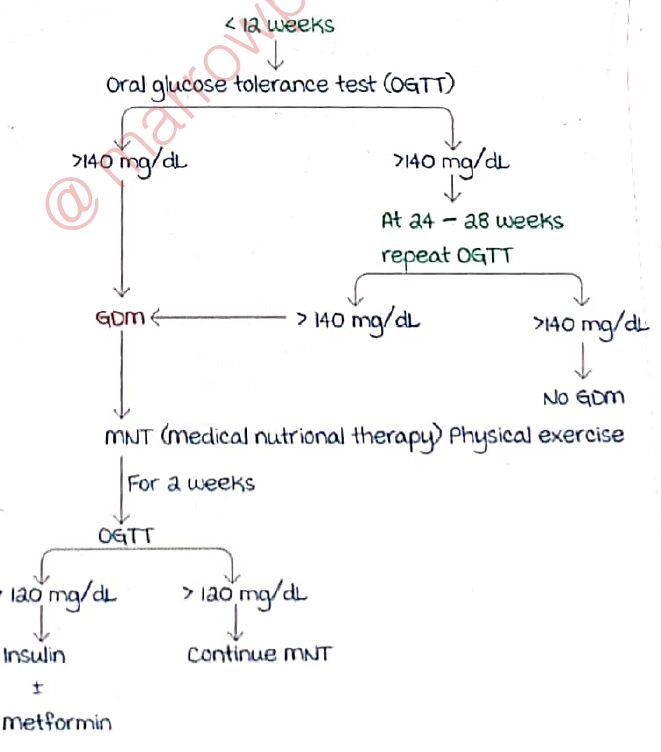
This flowchart gives a great overview of how we step up treatment. Remember, for the UKMLA, the key is knowing when to jump straight to insulin (fasting > 7.0 or > 6.0 with complications).
One last high-yield point for the AKT: Post-natal follow-up.
- Stop all diabetic meds immediately after birth.
- Check fasting glucose at 6–13 weeks post-partum (or HbA1c after 13 weeks).
- Advise on annual HbA1c checks because these women have a significantly higher risk of developing Type 2 Diabetes later in life.
Would you like to try a quick quiz on these NICE criteria to see if they've stuck?
Setting up chat...