Gender-affirming care: hormonal therapy, surgical options and guidelines
Gender-affirming care is such an important and evolving field of medicine. It's all about providing patient-centered care that aligns a person's physical characteristics with their gender identity, which can significantly improve mental health and quality of life.
To get us started, I'll pull up some high-yield lessons that cover the clinical side of these transitions.
📚 Gender-Affirming Care Lessons
The cornerstone of medical transition is often Gender-Affirming Hormone Therapy (GAHT). The goal is to induce physical changes that match a patient's gender identity by maintaining hormone levels in the physiological range of the affirmed gender.
1. Hormonal Therapy
Feminizing Therapy (Transfeminine)
- Estrogens: Usually 17-beta estradiol (oral, patch, or injection). It promotes breast development, softens skin, and redistributes fat to a more feminine pattern.
- Anti-androgens: Used to suppress endogenous testosterone.
- Spironolactone: Most common in the US (potassium-sparing diuretic with anti-androgenic effects).
- Cyproterone acetate: Common outside the US (progestin with strong anti-androgenic effects).
- GnRH Agonists: (e.g., Leuprolide) The "gold standard" but expensive; they shut down the HPG axis entirely.
Masculinizing Therapy (Transmasculine)
- Testosterone: Administered via intramuscular or subcutaneous injection, or transdermal gels/patches.
- Effects: Voice deepening, facial/body hair growth, increased muscle mass, and cessation of menses (amenorrhea).
I've put together a quick comparison table of the expected changes and timelines for you to visualize how this typically progresses.
| Effect | Expected Onset | Expected Maximum |
|---|---|---|
| Feminizing | ||
| Softening of skin | 3–6 months | Unknown |
| Breast growth | 3–6 months | 2–3 years |
| Fat redistribution | 3–6 months | 2–5 years |
| Decreased muscle mass | 3–6 months | 1–2 years |
| Masculinizing | ||
| Skin oiliness/acne | 1–6 months | 1–2 years |
| Facial/body hair growth | 3–6 months | 3–5 years |
| Scalp hair loss | >12 months | Variable |
| Voice deepening | 3–12 months | 1–2 years |
| Fat redistribution | 3–6 months | 2–5 years |
Beyond hormonal therapy, many patients choose surgical interventions to further align their physical appearance with their gender identity.
2. Surgical Options
Top Surgery (Chest)
- Masculinizing: Subcutaneous mastectomy with chest wall contouring. Techniques vary based on breast size (e.g., double incision with nipple grafts vs. "keyhole" for smaller chests).
- Feminizing: Breast augmentation (mammoplasty) using implants or fat grafting.
Bottom Surgery (Genital)
- Feminizing:
- Vaginoplasty: Creation of a vaginal canal and vulva (often using penile/scrotal skin inversion).
- Vulvoplasty: Creation of external female genitalia without a vaginal canal ("zero-depth").
- Masculinizing:
- Phalloplasty: Creation of a penis using a skin flap (often from the forearm or thigh). This usually involves multiple stages including urethral lengthening and scrotoplasty.
- Metoidioplasty: Creating a smaller phallus from the clitoris (which has been enlarged by testosterone).
Ancillary Procedures
- Facial Feminization Surgery (FFS): Includes brow bone reduction, rhinoplasty, and jaw contouring.
- Chondrolaryngoplasty: Commonly known as a "tracheal shave" to reduce the prominence of the Adam's apple.
- Voice Surgery: Procedures like thyroplasty to raise the pitch of the voice.
3. Guidelines and Standards of Care
The World Professional Association for Transgender Health (WPATH) publishes the Standards of Care (SOC), with Version 8 being the most recent update.
Key takeaways from the guidelines include:
- Informed Consent Model: Moving away from strict "gatekeeping" and focusing on the patient's autonomy and understanding of the risks and benefits.
- Multidisciplinary Care: Coordination between primary care, endocrinology, mental health professionals, and surgeons.
- Mental Health Assessment: While no longer always a requirement for hormone therapy in some models, a mental health assessment is still standard for surgical procedures to ensure the patient has adequate support and realistic expectations.
I'll search for a clinical flowchart that outlines the typical pathway for gender-affirming care to give you a better sense of the process.
This flowchart illustrates the multidisciplinary pathway for gender-affirming surgery (GAS), starting from the initial contact and eligibility screening based on WPATH SOC, through the consultation and pre-surgical phases, to the surgery and follow-up care.
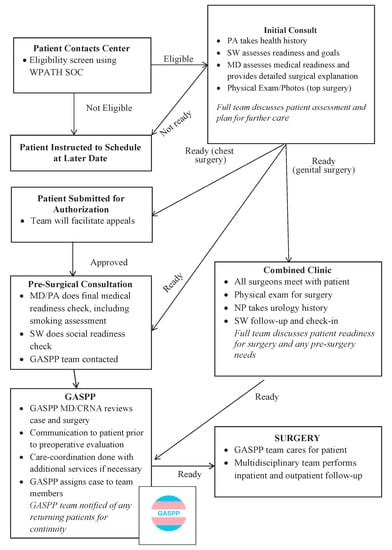
This multidisciplinary approach ensures that patients receive comprehensive care that addresses their physical, emotional, and social needs throughout their transition.
Key Takeaways for Exams:
- WPATH SOC 8 is the current standard for gender-affirming care.
- Feminizing therapy typically involves estrogen and anti-androgens (like spironolactone).
- Masculinizing therapy relies on testosterone, which can lead to erythrocytosis (monitor hematocrit!).
- Surgical options are diverse and tailored to the individual's goals, often requiring a period of hormone therapy and mental health support beforehand.
If you'd like to dive deeper into any of these specific surgeries or the side effects of hormone therapy, just let me know!
Setting up chat...