Gallstone disease: biliary colic, cholecystitis, cholangitis and management
Gallstone disease is a classic "bread and butter" topic for the UKMLA AKT, and it's really all about understanding the spectrum of how a tiny stone can cause a whole lot of trouble depending on where it gets stuck.
To get us started, I'll pull up some of the most relevant lessons from our library that cover everything from the basic pathophysiology to the latest NICE management guidelines.
📚 Gallstone Disease Lessons
It's super helpful to think of these conditions as a progression. Biliary colic is the "warning shot," cholecystitis is the "inflammation," and cholangitis is the "emergency."
I've put together a comparison table to help you quickly distinguish between them based on clinical presentation and lab findings—this is exactly how they'll test you in the AKT.
| Feature | Biliary Colic | Acute Cholecystitis | Ascending Cholangitis |
|---|---|---|---|
| Pathology | Transient cystic duct obstruction | Persistent cystic duct obstruction + Inflammation | CBD obstruction + Infection (Biliary stasis) |
| Pain | RUQ/Epigastric, "colicky" (comes and goes), post-prandial | Constant RUQ pain, may radiate to right shoulder | RUQ pain (part of Charcot's Triad) |
| Fever/Rigors | Absent | Present (Low grade) | Present (High grade/Rigors) |
| Jaundice | Absent | Usually absent | Present (Obstructive pattern) |
| Murphy's Sign | Negative | Positive | Negative/Variable |
| Inflammatory Markers (CRP/WCC) | Normal | Elevated | Markedly Elevated |
| Liver Function Tests (LFTs) | Normal | Usually normal (may have mild derangement) | Obstructive pattern (High Bilirubin, High ALP/GGT) |
| Management | Elective Cholecystectomy | NBM, Fluids, Antibiotics, Cholecystectomy (within 72h per NICE) | Emergency! IV Fluids, Antibiotics, Biliary decompression (ERCP) |
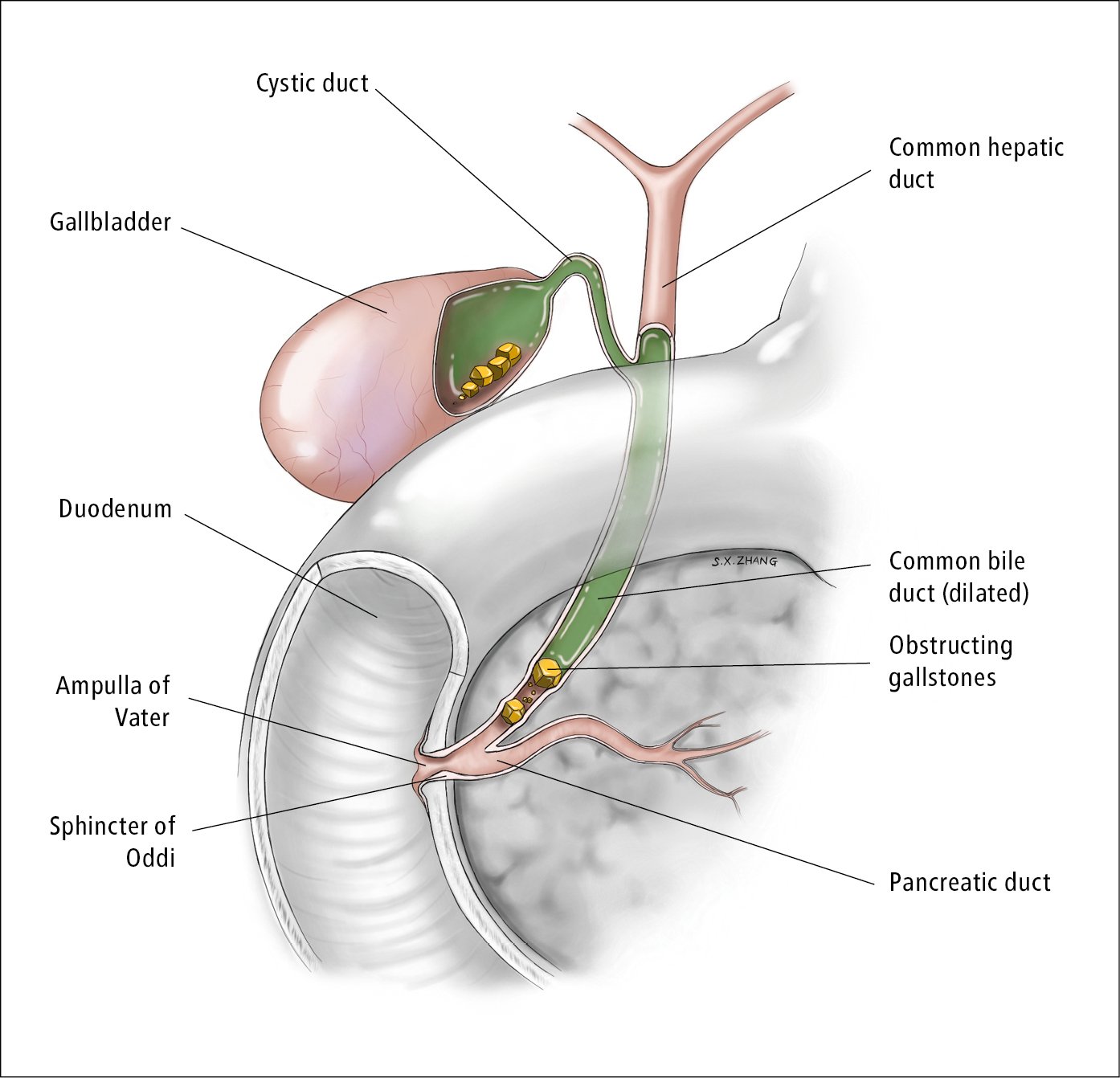
Visualizing where the stones are actually sitting makes the symptoms much easier to remember. For example, if a stone is in the cystic duct, you get cholecystitis, but if it's in the common bile duct (CBD), you get jaundice and potentially cholangitis.
Let me find a diagram of the biliary tree to show you exactly what I mean.
This diagram is perfect—it shows exactly how stones in the common bile duct (choledocholithiasis) can lead to that obstructive jaundice and potential cholangitis we were talking about.
Finally, let's look at the management pathway. A key "hot topic" for the AKT is the timing of surgery for acute cholecystitis. NICE guidelines recommend an early laparoscopic cholecystectomy (usually within 72 hours of presentation) rather than waiting for the inflammation to settle.
Here's a simplified management algorithm to help you keep the steps straight during the exam.
The key to mastering this for the AKT is recognizing that Ascending Cholangitis is a surgical emergency requiring urgent biliary decompression (usually via ERCP), while Acute Cholecystitis is an inflammatory condition that needs early surgery.
Remember the "Triads" and "Pentads" for your exams:
- Charcot's Triad (Cholangitis): RUQ pain + Fever + Jaundice.
- Reynold's Pentad (Severe Cholangitis): Charcot's Triad + Hypotension + Altered Mental Status.
If you're feeling confident with the theory, we could try a few practice questions to see how these scenarios pop up in the AKT!
Setting up chat...