Epilepsy management in primary care: drug choice, DVLA rules and women of childbearing age
Epilepsy is a massive topic for the AKT, and honestly, it's one of those areas where the guidelines have shifted quite a bit recently—especially regarding safety in women. It's all about matching the right drug to the right seizure type while keeping the patient's lifestyle and safety in mind.
I'll start by pulling up some high-yield lessons that cover these specific UK guidelines for you.
📚 Epilepsy Management Lessons
When it comes to picking the right drug, the "old school" way was always Valproate for everything generalized, but the NICE guidelines have shifted to be much more cautious. For focal seizures, your go-to first-line options are now Levetiracetam or Lamotrigine. For generalized tonic-clonic seizures, it's still Sodium Valproate for males, but for anyone with childbearing potential, we lean towards Levetiracetam or Lamotrigine first.
Let me find a clear comparison table for these drug choices and the specific DVLA rules, as they are super high-yield for the AKT.
Managing epilepsy in primary care requires a careful balance of clinical safety and legal requirements. Here is a breakdown of the key areas you'll need for the AKT.
1. Drug Choice (NICE Guidelines)
The choice depends heavily on the seizure type and the patient's sex/age:
- Focal Seizures:
- 1st line:
LevetiracetamorLamotrigine. - 2nd line:
CarbamazepineorZonisamide.
- 1st line:
- Generalized Tonic-Clonic Seizures (GTCS):
- 1st line:
Sodium Valproate(males and females not of childbearing potential). - 1st line for females of childbearing potential:
LevetiracetamorLamotrigine.
- 1st line:
- Absence Seizures:
EthosuximideorSodium Valproate. - Myoclonic Seizures:
Sodium Valproate(avoidLamotrigineas it can worsen myoclonus!).
2. Women of Childbearing Age
This is a high-priority safety area in the UK.
- Sodium Valproate: Must never be started in women of childbearing potential unless other treatments are ineffective or not tolerated. If used, the Pregnancy Prevention Programme (PPP) is mandatory (annual risk forms and highly effective contraception).
- Folic Acid: All women on AEDs should take
5mgdaily if they are planning a pregnancy (or even if there's a chance of one). - Contraception Interactions:
- Enzyme Inducers (e.g., Carbamazepine, Phenytoin, Phenobarbital) reduce the effectiveness of the COCP, POP, patch, and implant.
- Safe options: IUD (Copper), IUS (Mirena), and Depo-Provera are not affected by enzyme inducers.
3. DVLA Rules
Patients have a legal duty to inform the DVLA.
| Scenario | Driving Restriction |
|---|---|
| First Unprovoked Seizure | 6 months off (if no high-risk features on EEG/MRI). |
| Established Epilepsy | 12 months seizure-free. |
| Withdrawal of Medication | No driving during withdrawal and for 6 months after the last dose. |
| One-off Seizure with high risk | 12 months off. |
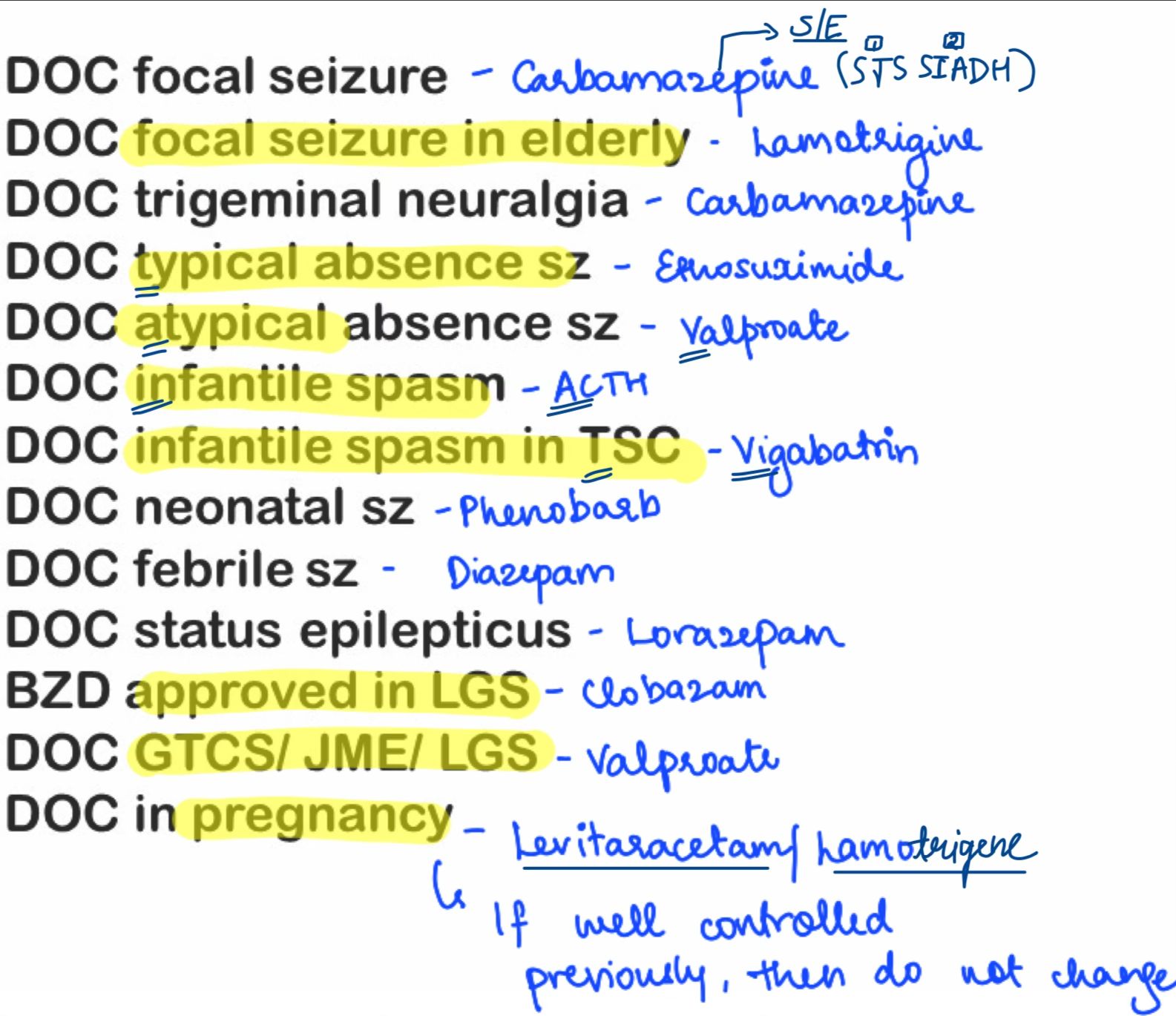
I've also found a quick reference for seizure-specific drug choices below:
That summary covers the core "must-knows" for your primary care rotations and the AKT. Remember that the Valproate Pregnancy Prevention Programme is a major focus for the GMC and the DVLA rules are non-negotiable—patients often ask about them first!
Would you like to try a few practice questions to see how these rules appear in exam scenarios?
Setting up chat...