Endometriosis: clinical features, laparoscopy and medical management
Endometriosis is one of those conditions that can be incredibly frustrating for patients because the symptoms often overlap with so many other things. It's essentially when tissue similar to the lining of the uterus (the endometrium) starts growing in places it shouldn't, like the ovaries, fallopian tubes, or the lining of the pelvis.
Since you're prepping for the UKMLA AKT, it's important to focus on the "classic" presentation and the gold-standard diagnostic steps.
Clinical Features
The symptoms are often cyclical, but as the condition progresses, the pain can become constant. Look out for these "Ds":
- Dysmenorrhea: Painful periods, often starting a few days before the bleed.
- Dyspareunia: Deep pain during or after intercourse.
- Dysuria/Dyschezia: Pain when passing urine or opening bowels (especially during the period).
- Chronic Pelvic Pain: Persistent pain lasting >6 months.
- Subfertility: Often the reason the condition is discovered during investigations.
Laparoscopy: The Gold Standard
While an ultrasound might show an "endometrioma" (a chocolate cyst on the ovary), a diagnostic laparoscopy is the definitive gold standard for diagnosis.
- It allows for direct visualization of deposits (often described as "gunpowder" or "cigarette burn" lesions).
- The big advantage is that it's "see and treat"—surgeons can biopsy, ablate, or excise the lesions during the same procedure.
Medical Management
The goal here is to suppress ovulation and thin the endometrial lining. We usually follow a stepped approach:
- Analgesia: NSAIDs (like Ibuprofen or Naproxen) and Paracetamol for symptomatic relief.
- Hormonal Treatment (First-line): Combined Oral Contraceptive Pill (COCP) or Progestogens (like the POP, Nexplanon, or the Mirena IUS).
- GnRH Agonists: (e.g., Leuprorelin) These induce a "pseudomenopause" by shutting down estrogen production. They are usually reserved for more severe cases and often require "add-back" HRT to protect bone density and manage side effects.
I'll pull up some high-yield lessons and a flowchart to help you visualize the management pathway, as the AKT loves testing the "next best step."
📚 Endometriosis Lessons
I've found a great management algorithm that perfectly summarizes the decision-making process for suspected endometriosis. It highlights when to start with medical therapy and when to jump straight to laparoscopy.
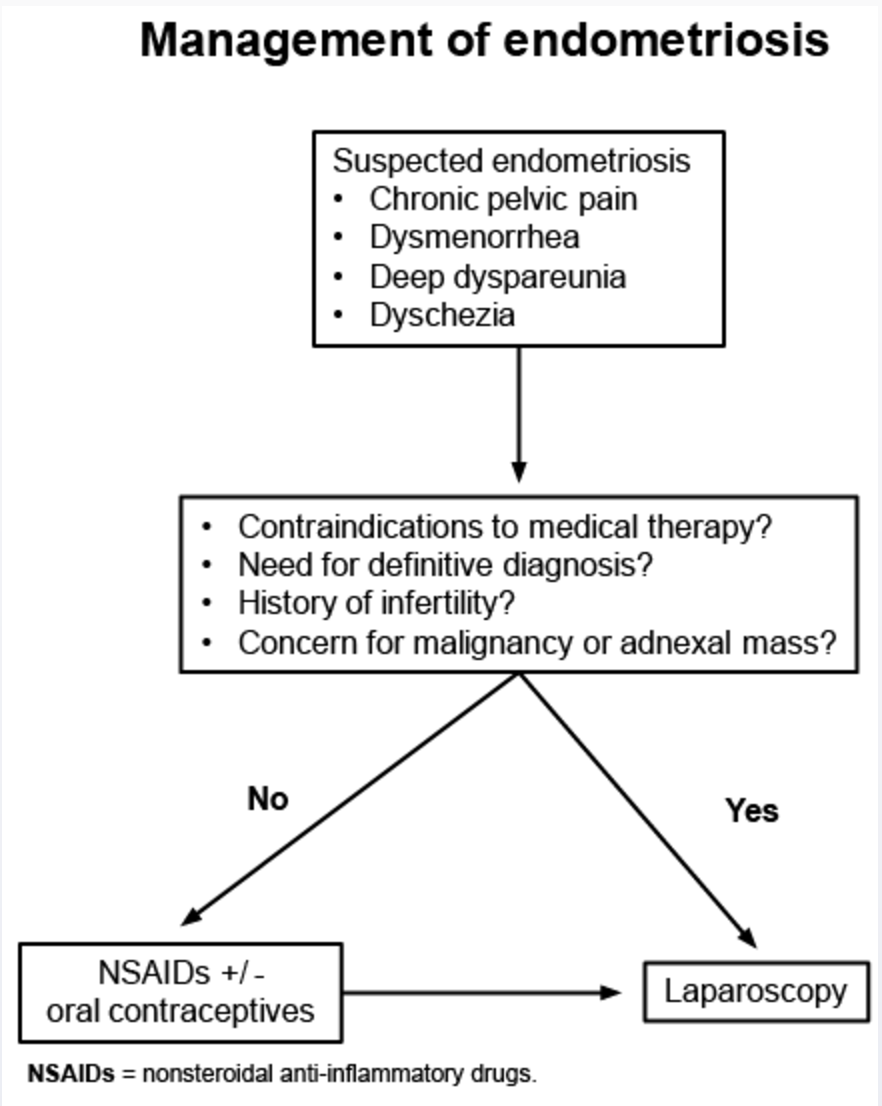
This flowchart is a great summary of the NICE guidelines approach. Notice how it emphasizes that if there's a history of infertility or a concern for malignancy, we move straight to laparoscopy rather than trying medical management first.
To help you lock this in, would you like to try a few practice questions or some flashcards on the medical management steps?
Setting up chat...