Endocrine surgery: thyroidectomy, parathyroid and adrenal surgery indications
Endocrine surgery is such a high-yield area, especially for NEET-PG and INI-CET! It’s all about knowing exactly when the medical management ends and the scalpel takes over.
Let's break down the surgical indications for the "Big Three": the thyroid, parathyroids, and adrenals. I'll start by pulling up some relevant lessons for you to dive deeper into later.
[tool call: get_related_lessons_by_search_query]
📚 Endocrine Surgery Lessons
Those lessons are a great place to start! Now, let's get into the nitty-gritty of the surgical indications.
1. Thyroidectomy
Surgery on the thyroid is generally indicated for three main reasons: Malignancy, Compression, or Hyperthyroidism that isn't responding to other treatments.
- Malignancy (Suspected or Confirmed): Any biopsy (FNAC) showing Bethesda IV, V, or VI (Follicular neoplasm, Suspicious for malignancy, or Malignant).
- Compressive Symptoms: A large goiter causing "the 3 Ds": Dyspnea (tracheal compression), Dysphagia (esophageal compression), or Dysphonia (recurrent laryngeal nerve involvement).
- Hyperthyroidism:
- Graves' Disease: If medical therapy (antithyroid drugs) fails, or if the patient has severe ophthalmopathy (where radioactive iodine is contraindicated).
- Toxic Multinodular Goiter (TMNG) or Toxic Adenoma: Surgery is often preferred over long-term meds.
- Cosmetic/Retrosternal Extension: Even if asymptomatic, a retrosternal goiter is usually removed because it will eventually cause trouble in the tight space of the mediastinum.
2. Parathyroid Surgery
The goal here is almost always to treat Primary Hyperparathyroidism (PHPT). If the patient has symptoms (the classic "Stones, Bones, Abdominal Groans, and Psychic Overtones"), surgery is a no-brainer.
However, the asymptomatic patients are the ones examiners love to test. Here are the NIH criteria for surgery in asymptomatic PHPT:
[tool call: show_markdown_to_user]
| Criterion | Threshold for Surgery |
|---|---|
| Age | < 50 years |
| Serum Calcium | > 1.0 mg/dL above the upper limit of normal |
| Skeletal Health | T-score ≤ -2.5 at any site (spine, hip, or radius) OR vertebral fracture |
| Renal Function | Creatinine Clearance (eGFR) < 60 mL/min |
| Renal Stones | Presence of stones or nephrocalcinosis on imaging |
| 24h Urine Calcium | > 400 mg/day (relative indication) |
3. Adrenal Surgery
Adrenalectomy is generally indicated for functional tumors (those producing hormones) or suspicious masses.
- Functional Tumors:
- Pheochromocytoma: (The "10% tumor") — always surgical after proper alpha and beta blockade.
- Cushing's Syndrome: If the source is an adrenal adenoma or carcinoma.
- Conn's Syndrome (Primary Hyperaldosteronism): If it's a unilateral adenoma (bilateral hyperplasia is usually managed medically).
- Non-Functional Masses (Incidentalomas):
- Size: Any mass > 4 cm is usually removed because the risk of adrenocortical carcinoma (ACC) increases significantly.
- Imaging Features: High Hounsfield units (> 10 HU on non-contrast CT), slow washout, or irregular borders.
- Growth: Any mass that grows by > 1 cm during follow-up.
I'll find a diagram of the adrenal gland to help you visualize where these tumors typically arise.
[tool call: assetSearch]
This diagram is perfect for visualizing the different zones of the adrenal gland and the tumors that arise from them.
[tool call: show_markdown_to_user]
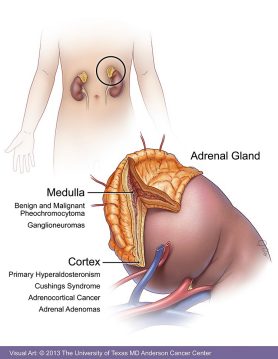
That diagram really helps to see how the cortex and medulla are distinct, which explains why the symptoms of a pheochromocytoma (medulla) are so different from Cushing's (cortex).
To wrap it all up, here’s a quick high-yield mnemonic for the "6 S's" of adrenal surgery:
The 6 S's of Adrenalectomy:
- Secreting (Functional tumors)
- Size (> 4 cm)
- Suspicious (Imaging features)
- Speed (Rapid growth > 1 cm/year)
- Symptoms (Pain, pressure)
- Secondary (Metastatic disease)
I hope this helps you master these endocrine surgery indications! If you're ready to test your knowledge, I can set up a quick quiz for you. Just let me know!
Setting up chat...