Endocrine pathology: thyroid nodules, adrenal tumors and pituitary adenomas
Endocrine pathology is a huge part of the NEET-PG and INI-CET exams because it connects so many clinical dots! Let's break down these three heavy hitters: thyroid nodules, adrenal tumors, and pituitary adenomas.
1. Thyroid Nodules
Most thyroid nodules are benign (like follicular adenomas), but we always worry about malignancy. The diagnostic gold standard is Fine Needle Aspiration (FNA), which we classify using the Bethesda System.
- Papillary Carcinoma: The most common type. Look for
==Orphan Annie eye nuclei==(clearing of chromatin) and Psammoma bodies. It has an excellent prognosis and spreads via lymphatics. - Follicular Carcinoma: Unlike papillary, this spreads via the blood (hematogenous). You can't diagnose this on FNA because you need to see capsular or vascular invasion to distinguish it from an adenoma.
- Medullary Carcinoma: Arises from Parafollicular C-cells and secretes Calcitonin. It's associated with MEN 2A and 2B (RET oncogene).
- Anaplastic Carcinoma: Seen in the elderly; highly aggressive with a very poor prognosis.
2. Adrenal Tumors
We divide these based on where they arise: the cortex or the medulla.
- Adrenal Adenoma: Often "incidentalomas." They can be functional, causing Cushing’s Syndrome (cortisol) or Conn’s Syndrome (aldosterone).
- Adrenal Cortical Carcinoma: Usually large (>6cm) and more likely to be functional (often causing virilization).
- Pheochromocytoma: Arises from the adrenal medulla (chromaffin cells). Remember the Rule of 10s: 10% bilateral, 10% malignant, 10% extra-adrenal, and 10% familial. It presents with the classic triad:
==Episodic headache, sweating, and palpitations==.
3. Pituitary Adenomas
These are usually benign but cause trouble by either secreting hormones or pressing on nearby structures (like the optic chiasm, causing bitemporal hemianopia).
- Prolactinoma: The most common functional adenoma. Causes galactorrhea, amenorrhea, and decreased libido.
- Somatotroph Adenoma: Secretes Growth Hormone (GH), leading to Acromegaly in adults or Gigantism in children.
- Corticotroph Adenoma: Secretes ACTH, leading to Cushing’s Disease.
I'll pull up some high-yield lessons so you can explore the histology and management of these conditions in more detail.
📚 Endocrine Pathology Lessons
Those lessons will give you the deep dive you need, especially for the histology and staging.
To help you visualize the differences between the types of thyroid cancer—which is a very common exam topic—I'm going to pull up a comparison diagram for you.
This image provides a great histopathological overview of the different thyroid cancers, from the well-differentiated papillary types to the highly aggressive anaplastic variant.
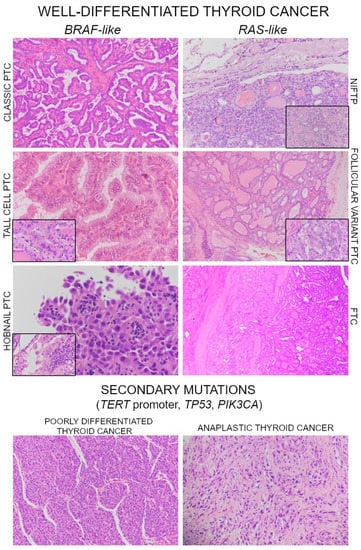
That histopathology image is a great way to see the differences between the well-differentiated types (like Papillary and Follicular) and the highly aggressive Anaplastic carcinoma.
If you're ready to test your knowledge on these endocrine topics, I can set up a custom quiz or some flashcards for you. Just let me know which one you'd prefer!
Setting up chat...