Emergency contraception: options, time limits and eligibility
Emergency contraception (EC) is a high-yield topic for the UKMLA AKT, and it's one of those areas where the clinical nuances—like BMI and drug interactions—really matter.
The most important thing to remember right off the bat is that the Copper Intrauterine Device (Cu-IUD) is the most effective form of EC and should be offered to all patients, regardless of their BMI.
I've put together a comparison table of the three main options used in the UK to help you keep the timeframes and eligibility criteria straight.
| Feature | Copper IUD (Cu-IUD) | Ulipristal Acetate (UPA - e.g., ellaOne) | Levonorgestrel (LNG - e.g., Levonelle) |
|---|---|---|---|
| Time Limit | Up to 120 hours (5 days) after UPSI OR up to 5 days after the earliest expected ovulation. | Up to 120 hours (5 days) after UPSI. | Up to 72 hours (3 days) after UPSI. |
| Effectiveness | >99% (Most effective) | More effective than LNG, especially between 72-120 hours. | Less effective than UPA/IUD, effectiveness decreases over time. |
| BMI Considerations | No restriction. | Effectiveness may be reduced if BMI >30kg/m² or weight >85kg. | Effectiveness reduced if BMI >26kg/m² or weight >70kg (consider double dose). |
| Breastfeeding | Safe to use. | Avoid breastfeeding for 1 week after taking. | Safe to use. |
| Key Contraindications | Current PID, unexplained vaginal bleeding, Wilson's disease. | Severe asthma controlled by oral glucocorticoids, severe hepatic impairment. | None absolute, but less effective if used late. |
| Drug Interactions | None. | Reduced by enzyme inducers; avoid if taken progestogens in the last 7 days. | Reduced by enzyme inducers (requires double dose: 3mg). |
That table covers the basics, but there are a few "exam-favorite" nuances you should keep in mind for the AKT:
- The IUD "Earliest Expected Ovulation" Rule: This is a classic. You can fit a Cu-IUD up to 5 days after the earliest expected date of ovulation, even if that's more than 5 days after Unprotected Sexual Intercourse (UPSI). For a standard 28-day cycle, ovulation is day 14, so you could technically fit it up to day 19.
- The UPA and Progestogen Clash: Ulipristal Acetate (UPA) is a selective progesterone receptor modulator. If a patient takes UPA and then immediately starts a progestogen-containing contraceptive (like the pill), the progestogen can actually make the UPA less effective. The current FSRH guidance is to wait 5 days after taking UPA before starting hormonal contraception.
- Enzyme Inducers: If a patient is on enzyme-inducing drugs (like carbamazepine or St John's Wort), oral EC is much less effective. The Cu-IUD is the gold standard here. If they refuse the IUD, they need a double dose of Levonorgestrel (3mg). UPA is not recommended for those on enzyme inducers.
I'll pull up some specific lessons on this so you can dive deeper into the FSRH algorithms.
📚 Emergency Contraception Lessons
Those lessons will give you the deep dive you need, especially on the pharmacology side.
One last thing to keep in mind for clinical scenarios: Fraser Guidelines. If you're dealing with a patient under 16, you'll need to assess their competency to consent to contraception without parental involvement. It's a common crossover topic between O&G and Ethics.
Let me see if I can find a helpful flowchart or diagram to help you visualize the decision-making process for choosing between the different EC methods.
This infographic provides a great summary of the different options, including the weight-based efficacy notes we discussed. It's a handy visual to keep in mind when you're trying to decide between the oral options and the IUD in a clinical scenario.
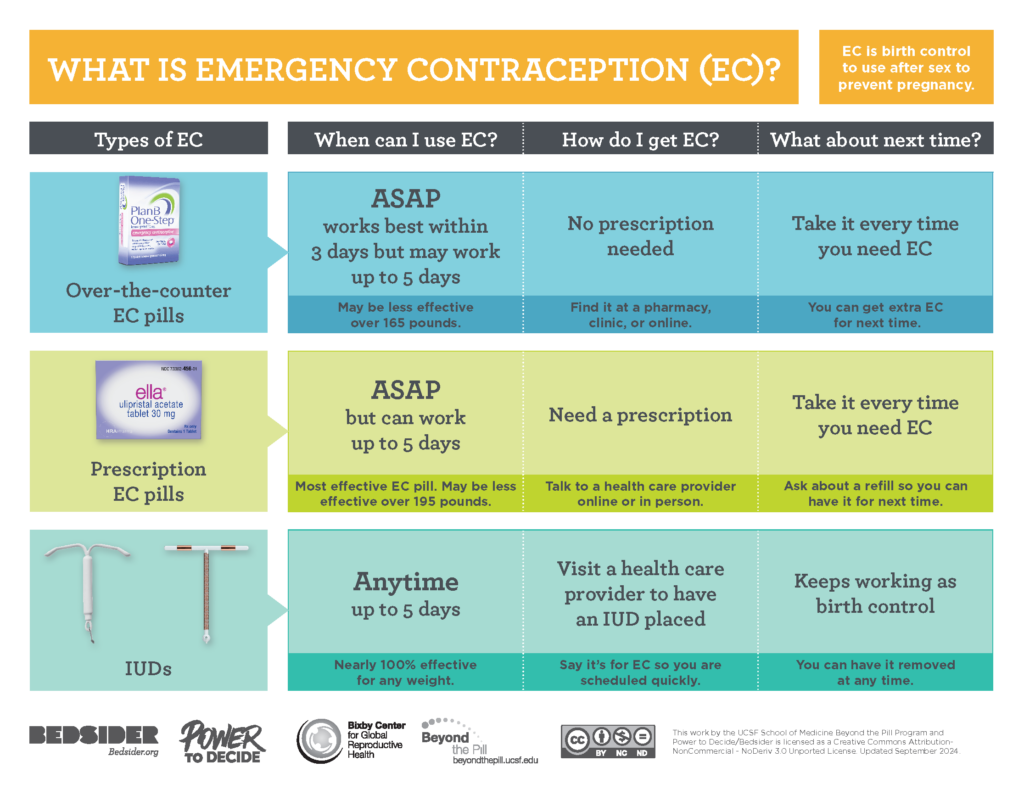
That chart really highlights how the IUD is the "gold standard" for effectiveness.
Just a final clinical tip for your exams: always advise the patient to perform a pregnancy test in 3 weeks (or if their next period is more than 7 days late, or lighter/shorter than usual), even if they've used EC correctly. And of course, use the opportunity to discuss ongoing contraception and STI screening!
Let me know if you want to dive into any of those specific drug interactions or the "quick start" rules for regular contraception.
Setting up chat...