Eating disorders: anorexia nervosa, bulimia — diagnosis, complications and treatment
Eating disorders are such a critical topic, not just for the exams but because they have some of the highest mortality rates in psychiatry. It's really all about distinguishing the patient's BMI and their specific behaviors.
Anorexia Nervosa (AN)
The hallmark of Anorexia is a significantly low body weight (BMI < 18.5 kg/m²) driven by an intense fear of gaining weight and a distorted perception of body shape.
- Subtypes:
- Restricting: Weight loss through dieting, fasting, or excessive exercise.
- Binge-eating/purging: The patient also engages in intermittent bingeing or purging (vomiting, laxatives).
- Complications: This is where the "starvation physiology" kicks in. You'll see bradycardia, hypotension, lanugo hair (fine, downy hair), and amenorrhea. The most dangerous acute complication is Refeeding Syndrome, where a shift in electrolytes (especially hypophosphatemia) can lead to heart failure.
- Treatment: The absolute first priority is nutritional rehabilitation. Psychotherapy (like CBT) is essential. Interestingly, SSRIs like Fluoxetine aren't very effective until the patient has reached a healthier weight.
Bulimia Nervosa (BN)
Unlike Anorexia, patients with Bulimia usually have a normal or even high BMI. They experience recurrent episodes of binge eating followed by compensatory behaviors (purging, fasting, or excessive exercise) to prevent weight gain.
- Diagnosis: These episodes must occur at least once a week for 3 months.
- Complications: Look for the "purging signs": Russell sign (calluses on the knuckles), parotid gland enlargement, and dental enamel erosion from gastric acid. Lab-wise, you'll often find hypokalemia and metabolic alkalosis.
- Treatment: Cognitive Behavioral Therapy (CBT) is the gold standard here. Unlike in AN, Fluoxetine is FDA-approved and very effective in reducing the binge-purge cycle.
To help you visualize the clinical signs we just talked about, I'll find a diagram that highlights the physical manifestations of these disorders.
This diagram is perfect for visualizing the physical toll these disorders take on the body, especially the specific signs of purging like the Russell sign.
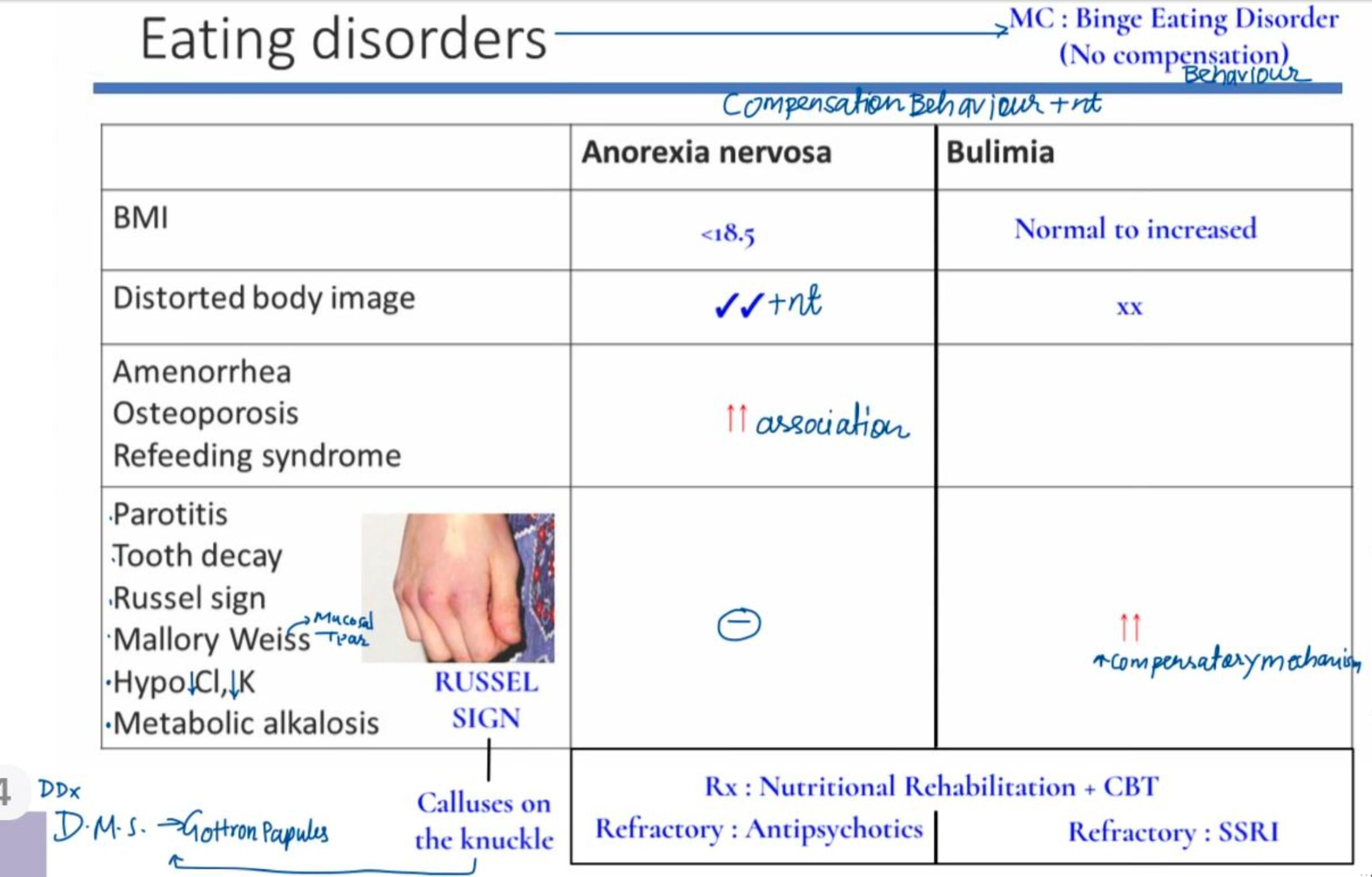
To make it easier for your revision, here is a quick comparison table of the key diagnostic and clinical differences between the two.
| Feature | Anorexia Nervosa | Bulimia Nervosa |
|---|---|---|
| Body Weight | Low BMI (<18.5 kg/m²) | Normal or Overweight |
| Core Behavior | Food restriction; may purge | Binge eating + Compensatory behavior |
| Body Image | Severely distorted | Overly influenced by weight |
| Physical Signs | Lanugo, bradycardia, amenorrhea | Parotid swelling, enamel erosion |
| Electrolytes | Refeeding (Low PO4) | Hypokalemia, Alkalosis |
| First-line Tx | Nutritional rehab + CBT | CBT |
| Pharmacotherapy | Olanzapine (if refractory) | Fluoxetine |
I've also pulled up some high-yield lessons that dive deeper into the psychiatric management and the specific DSM-5 criteria for these conditions.
📚 Eating Disorder Lessons
And to make sure you've got those key diagnostic features locked in, here are some flashcards for a quick active recall session.
🗂️ Eating Disorder Flashcards
Tap to study 26 flashcards in the Oncourse app
I hope this helps you get a clear handle on these eating disorders! They're high-yield for both psychiatry and internal medicine, so definitely keep an eye on those electrolyte imbalances and the BMI criteria.
If you're feeling ready to test your knowledge, I can set up a quick quiz for you, or we could even try a clinical case study game to see how you'd manage a patient in the clinic. Just let me know!
Setting up chat...