Diabetic emergencies: DKA vs HHS — comparison, diagnosis and management
Managing diabetic emergencies is a bread-and-butter skill for any junior doctor, especially when you're on a busy medical take. While both Diabetic Ketoacidosis (DKA) and Hyperosmolar Hyperglycemic State (HHS) involve a lack of effective insulin, they present quite differently on your blood gas and lab results.
I've put together a comparison table to help you distinguish between the two at a glance.
| Feature | Diabetic Ketoacidosis (DKA) | Hyperosmolar Hyperglycemic State (HHS) |
|---|---|---|
| Primary Patient | Usually Type 1 Diabetes | Usually Type 2 Diabetes (often elderly) |
| Onset | Rapid (< 24 hours) | Subacute (days to weeks) |
| Glucose | > 11.0 mmol/L (or known DM) | > 30.0 mmol/L |
| Ketones | Blood > 3.0 mmol/L or Urine ++ | Low/Absent (< 1.5 mmol/L) |
| pH | < 7.3 (Acidosis) | > 7.3 (Normal/Mildly reduced) |
| Bicarbonate | < 15.0 mmol/L | > 15.0 mmol/L |
| Osmolality | Variable | High (> 320 mOsm/kg) |
| Dehydration | Moderate | Severe |
Diagnosis
For DKA, you're looking for the "D-K-A" triad:
- Diabetes: Glucose > 11 mmol/L (or known DM).
- Ketosis: Blood ketones > 3.0 mmol/L or urine ketones ++.
- Acidosis: pH < 7.3 or bicarbonate < 15.0 mmol/L.
For HHS, the criteria focus on profound hyperglycemia and high osmolality:
- Hypovolemia
- Marked hyperglycemia (> 30 mmol/L)
- High serum osmolality (> 320 mOsm/kg)
- Note: Ketones are usually low, and pH is > 7.3.
Management Principles
The management of both conditions revolves around the same four pillars, but the speed and priorities differ.
- Fluid Resuscitation: This is the most critical step. In HHS, patients are often much more dehydrated (losing up to 10-20% of body weight), so fluid replacement must be careful to avoid rapid shifts in osmolality.
- Insulin Therapy:
- DKA: Fixed-rate intravenous insulin infusion (FRIII) is started immediately (0.1 units/kg/hr).
- HHS: Fluid replacement alone often drops glucose levels. Insulin is only started if glucose stops falling with fluids or if there are significant ketones.
- Potassium Replacement: Insulin drives potassium into cells. Even if the initial K+ is normal, it will drop rapidly once treatment starts.
- Treat the Trigger: Always look for the underlying cause—infection (UTI/Pneumonia), MI, or non-compliance with meds.
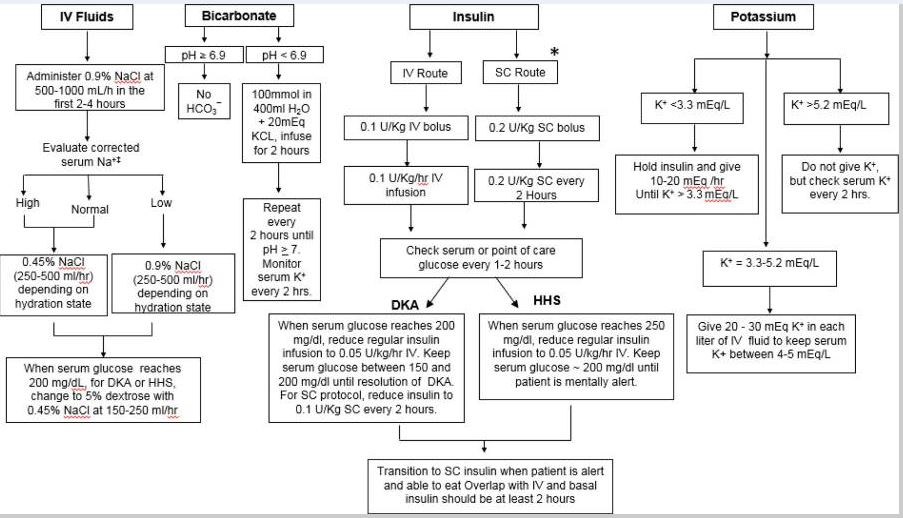
I'll find a diagram that illustrates the management algorithm for you.
This flowchart summarizes the key steps in managing both DKA and HHS, including fluid resuscitation, insulin administration, and potassium replacement.
To help you dive deeper into the specifics of these conditions, I've pulled up some high-yield lessons.
📚 Related Lessons: Diabetic Emergencies
Ready to test your knowledge? Here's a quick quiz on the diagnosis and management of these diabetic emergencies.
✍️ DKA vs HHS Quiz
Tap to practice questions in the Oncourse app
I hope this breakdown helps you feel more confident in distinguishing between DKA and HHS. Remember, the key is to check the ketones and pH early—that's what will guide your initial management.
If you have any more questions about these or any other endocrine emergencies, just let me know!
Setting up chat...