Building a differential diagnosis: systematic approach
Building a systematic differential diagnosis (DDx) is basically like being a medical detective. Instead of just guessing, you use frameworks to make sure you don't miss those "can't-miss" diagnoses. It's one of the most critical skills for the USMLE and clinical rotations!
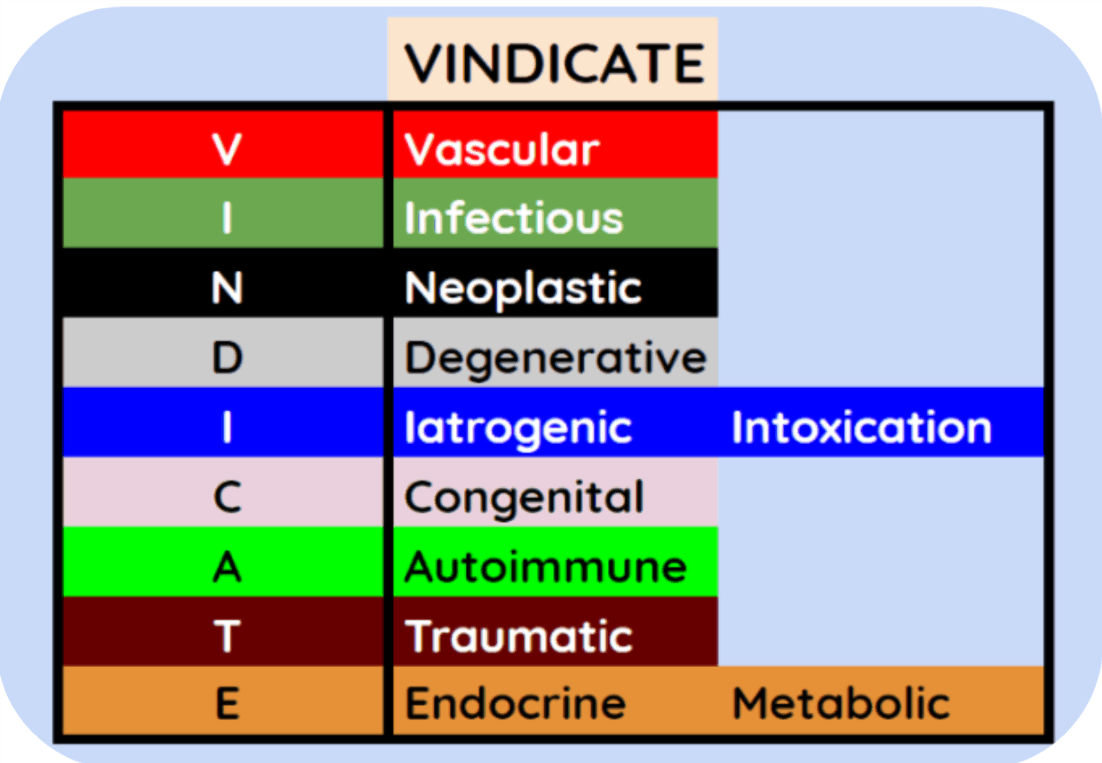
The most popular and reliable framework is the VINDICATE+ mnemonic. It helps you categorize potential causes by their underlying pathophysiology.
The VINDICATE+ Framework
- V – Vascular: Ischemia, hemorrhage, embolism (e.g., PE, MI, Stroke)
- I – Infectious: Bacterial, viral, fungal, parasitic (e.g., Pneumonia, Abscess)
- N – Neoplastic: Benign or malignant primary tumors, or metastases
- D – Degenerative/Deficiency: Osteoarthritis, Vitamin B12 deficiency, Alzheimer's
- I – Iatrogenic/Intoxication: Medication side effects, toxins, surgical complications
- C – Congenital: Hereditary conditions, structural heart defects
- A – Autoimmune/Allergic/Anatomic: Lupus, anaphylaxis, intussusception
- T – Traumatic: Fractures, concussions, burns
- E – Endocrine/Metabolic: Diabetes, thyroid issues, electrolyte imbalances
- + – Psychogenic: Somatization, conversion disorder
How to Build Your List
- Start with the Chief Complaint: Define the clinical problem (e.g., "Acute onset pleuritic chest pain").
- Gather the "Must-Haves": Use the patient's age, sex, and risk factors to narrow the VINDICATE list.
- Prioritize: Rank your list by Probability (what's most likely) vs. Severity (what's most dangerous).
- Refine: Use the history and physical exam to "rule in" or "rule out" items on your list.
I'll find a helpful visual to help you visualize this clinical reasoning process.
I've found a great visual breakdown of the VINDICATE mnemonic that you can use as a mental checklist during your clinical rotations.
This framework is a lifesaver when you're put on the spot by an attending! To help you dive deeper into how to apply this in real-world scenarios, I've pulled up some high-yield lessons on diagnostic reasoning.
📚 Clinical Reasoning Lessons
These lessons go into the "Hypothetico-deductive" model, which is the fancy way of saying you're constantly testing your theories as you get more info from the patient.
One pro-tip: always keep the "Can't-Miss" diagnoses at the top of your mental list, even if they aren't the most likely. For example, if a patient has chest pain, you must rule out an MI or PE before you settle on something like GERD.
Would you like to try a quick Clinical Rounds case to see how you'd apply this systematic approach to a real patient scenario? It's a great way to practice before your next shift!
Setting up chat...