Cytopathology: Pap smear classification, FNAC technique and interpretation
Cytopathology is such a high-yield area, especially for exams like NEET-PG and INI-CET! It’s basically the art of looking at individual cells to spot trouble before it becomes a full-blown tissue problem.
Let's start by pulling up some core lessons on these topics to give us a solid foundation.
📚 Cytopathology Lessons
The Bethesda System is the gold standard for reporting cervical cytology. It's designed to be clinically useful, telling the gynecologist exactly what the next step should be.
I've put together a summary table of the classification to make it easier to digest.
| Category | Description | Clinical Significance |
|---|---|---|
| NILM | Negative for Intraepithelial Lesion or Malignancy | Normal; may show organisms like Trichomonas or Candida. |
| ASC-US | Atypical Squamous Cells of Undetermined Significance | Most common abnormal finding; requires HPV testing or repeat Pap. |
| ASC-H | Atypical Squamous Cells - cannot exclude HSIL | Higher risk than ASC-US; usually warrants colposcopy. |
| LSIL | Low-grade Squamous Intraepithelial Lesion | Corresponds to CIN 1; often associated with transient HPV infection. |
| HSIL | High-grade Squamous Intraepithelial Lesion | Corresponds to CIN 2/3; high risk of progression to carcinoma. |
| SCC | Squamous Cell Carcinoma | Invasive cancer. |
Now, let's talk about Fine Needle Aspiration Cytology (FNAC). This is a quick, minimally invasive way to sample palpable masses (like thyroid nodules, breast lumps, or lymph nodes).
The FNAC Technique
The procedure is relatively straightforward but requires a bit of finesse:
- Equipment: A 22-25 gauge needle (thin!) and a 10-20 mL syringe, often held in a Franzen handle for better control.
- Procedure: The mass is stabilized with one hand, and the needle is inserted. Multiple passes are made in different directions without exiting the skin to get a representative sample.
- Suction: Negative pressure is applied while moving the needle. It's crucial to release the suction before withdrawing the needle to avoid sucking the sample into the syringe barrel (where it's hard to get out!).
- Smearing: The material is expelled onto a slide, smeared, and either air-dried (for Giemsa/Diff-Quik stains) or alcohol-fixed (for Papanicolaou/H&E stains).
Interpretation and Adequacy
When we look at the slides, the first thing we ask is: Is it adequate?
- Adequacy: This depends on the organ. For example, in a thyroid FNAC, we usually need at least 6 groups of well-preserved follicular cells (10 cells per group).
- Diagnostic Categories: Most FNAC reports follow a standardized system (like the Bethesda System for Thyroid or the Yokohama System for Breast):
- Inadequate/Non-diagnostic: Not enough cells or too much blood.
- Benign: No evidence of malignancy (e.g., a colloid goiter).
- Atypical/Suspicious: Cells look weird, but not quite "cancer" weird.
- Malignant: Clear evidence of cancer (e.g., Papillary Thyroid Carcinoma).
I'll find a diagram of the FNAC procedure to help you visualize the "suction and release" part, which is a common exam point!
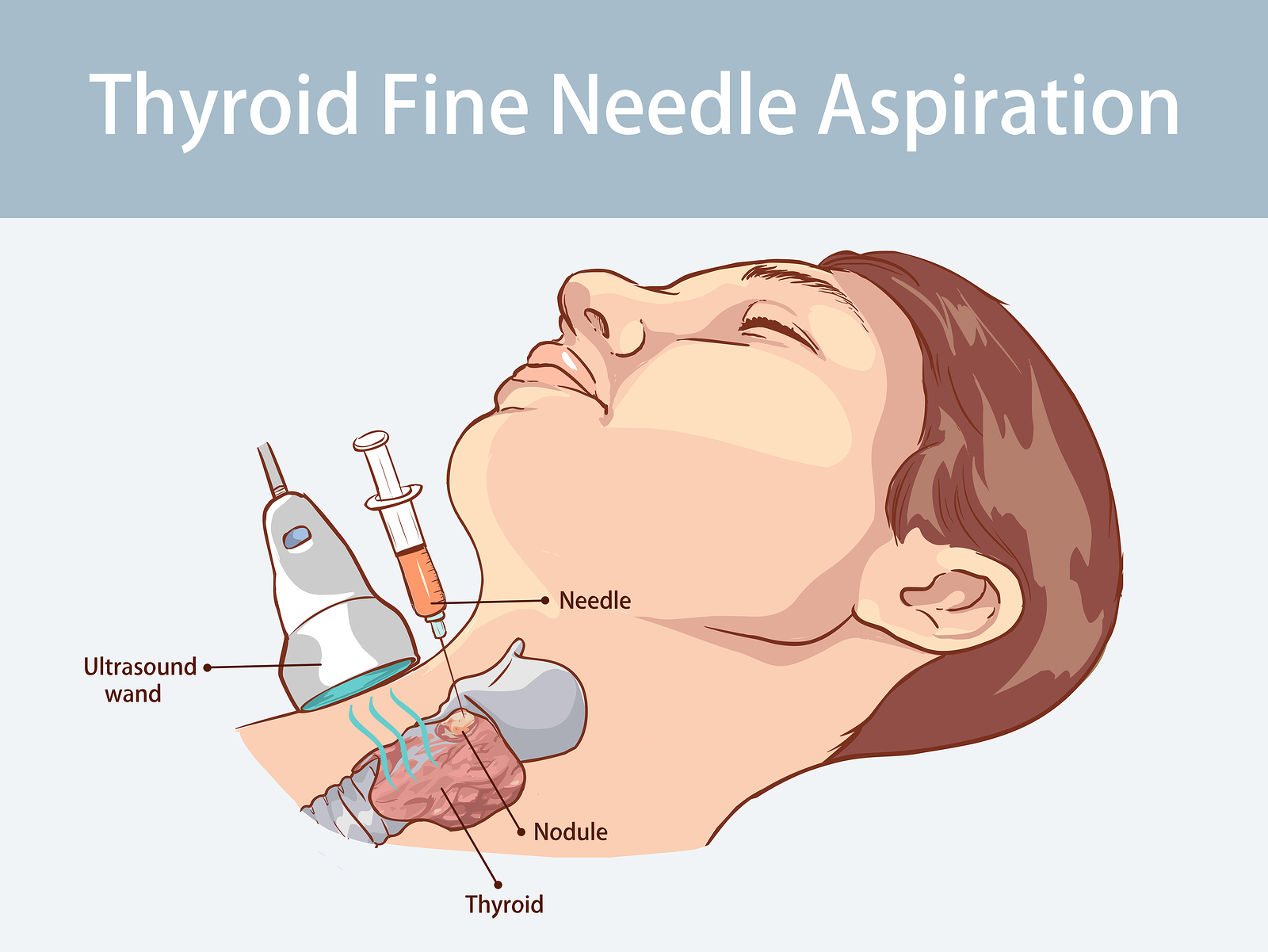
This illustration shows a thyroid FNAC being performed under ultrasound guidance, which is the gold standard for sampling non-palpable or complex nodules.
To wrap up, remember these high-yield pearls:
- Pap Smear: The Bethesda System is for reporting. LSIL is often transient, while HSIL is the one that really worries us.
- FNAC: It's a screening tool, not a definitive biopsy. If the FNAC is suspicious, the next step is usually a core biopsy or surgical excision.
- Staining: Pap stain is best for nuclear detail (great for cancer), while Giemsa is better for background material (like colloid or mucin).
Would you like to try a quick quiz on these concepts to see how much you've locked in?
Setting up chat...