Corticospinal tract: pathway, decussation and upper vs lower motor neuron lesions
Ah, the Corticospinal Tract (CST)! It's essentially the "interstate highway" for voluntary motor control. If you want to wiggle your toes or sign a check, this is the pathway doing the heavy lifting. For the USMLE, understanding exactly where this tract lives and where it crosses is high-yield territory.
The Pathway: From Cortex to Cord
The journey starts in the Primary Motor Cortex (Precentral Gyrus). The axons travel down through the Posterior Limb of the Internal Capsule—remember that specific location, as it's a favorite for "lacunar stroke" questions! From there, they descend through the brainstem:
- Midbrain: Through the cerebral peduncles (middle three-fifths).
- Pons: Scattered among the pontine nuclei.
- Medulla: They bunch back together to form the Pyramids.
I'll pull up a diagram so you can visualize this descent through the brainstem.
This diagram perfectly traces the path from the motor cortex down to the spinal cord. Notice how the fibers stay on the same side (ipsilateral) until they reach the very bottom of the medulla.
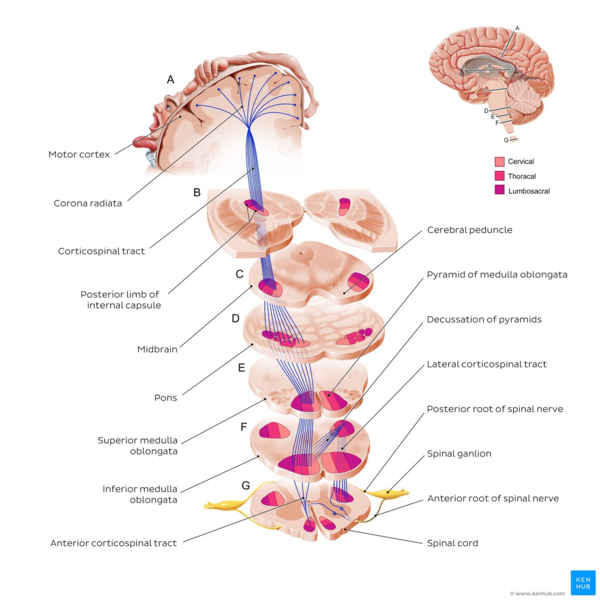
The Decussation: The Great Cross-Over
At the lower medulla, the tract hits the Pyramidal Decussation. This is where the magic happens:
- Lateral Corticospinal Tract (~90%): These fibers cross over to the opposite side. They control the distal muscles (like your hands and feet).
- Anterior Corticospinal Tract (~10%): These stay on the same side and only cross at the level of the spinal cord where they exit. They mostly handle proximal/axial muscles (your trunk).
UMN vs. LMN Lesions: The Clinical "Tell"
This is the bread and butter of neurology exams. Think of the Upper Motor Neuron (UMN) as the "manager" and the Lower Motor Neuron (LMN) as the "worker."
- If the manager (UMN) is gone, the worker goes wild (spasticity, high reflexes).
- If the worker (LMN) is gone, nothing happens (flaccidity, no reflexes).
Let me put this into a clear comparison table for you.
| Feature | Upper Motor Neuron (UMN) Lesion | Lower Motor Neuron (LMN) Lesion |
|---|---|---|
| Muscle Tone | Spasticity (Increased tone) | Flaccidity (Decreased tone) |
| Reflexes | Hyperreflexia (Brisk) | Hyporeflexia or Areflexia (Absent) |
| Atrophy | Minimal (Disuse only) | Severe (Denervation) |
| Fasciculations | Absent | Present (Twitching) |
| Babinski Sign | Positive (Upgoing toe) | Negative (Downgoing toe) |
| Paralysis | Spastic paralysis | Flaccid paralysis |
That table is your best friend for USMLE Step 1 and Step 2. If you see "upgoing toes" (Babinski sign) and "brisk reflexes," you're looking at a UMN lesion. If you see "fasciculations" (muscle twitches) and "wasting," it's an LMN lesion.
Let me find some relevant lessons for you to dive deeper into these concepts.
📚 Motor Pathway Lessons
Those lessons cover everything from the basic anatomy to clinical testing. I've also included a lesson on Amyotrophic Lateral Sclerosis (ALS) because it's the classic "both UMN and LMN" disease—definitely worth a look!
To help you lock in these differences, let's pull up some flashcards.
It looks like my first search for flashcards was a bit too specific. Let me try a broader search to find those high-yield cards for you.
🗂️ Motor Neuron Flashcards
Tap to study 23 flashcards in the Oncourse app
There we go! Those flashcards will help you drill the specifics, like where the anterior tract decussates (at the spinal cord level) versus the lateral tract (at the medulla).
To recap:
- Pathway: Motor cortex → Internal capsule (posterior limb) → Brainstem → Medulla.
- Decussation: 90% cross at the medulla (Lateral CST); 10% cross at the spinal cord (Anterior CST).
- Lesions: UMN = "Everything goes UP" (tone, reflexes, Babinski); LMN = "Everything goes DOWN" (tone, reflexes, muscle mass).
You've got this! Let me know if you want to tackle a specific clinical case or if you're ready to move on to another tract.
Setting up chat...