Diseases of the conjunctiva: allergic, infective conjunctivitis and pterygium
Ah, the conjunctiva! It’s basically the "security guard" of the eye, and when it gets grumpy, things get red and uncomfortable pretty fast. These topics are high-yield for your exams, especially distinguishing between the different types of "pink eye."
Let's start with Infective Conjunctivitis. It's usually a battle between bacteria and viruses:
- Bacterial Conjunctivitis: Think purulent (yellow-green) discharge and "stuck-together" eyelids in the morning. Common culprits are Staph aureus, Strep pneumoniae, and H. influenzae.
- Viral Conjunctivitis: Usually caused by Adenovirus. It’s super contagious! Look for watery discharge, follicles on the palpebral conjunctiva, and that classic preauricular lymphadenopathy.
I'll pull up some images so you can see the clinical differences between these and a pterygium.
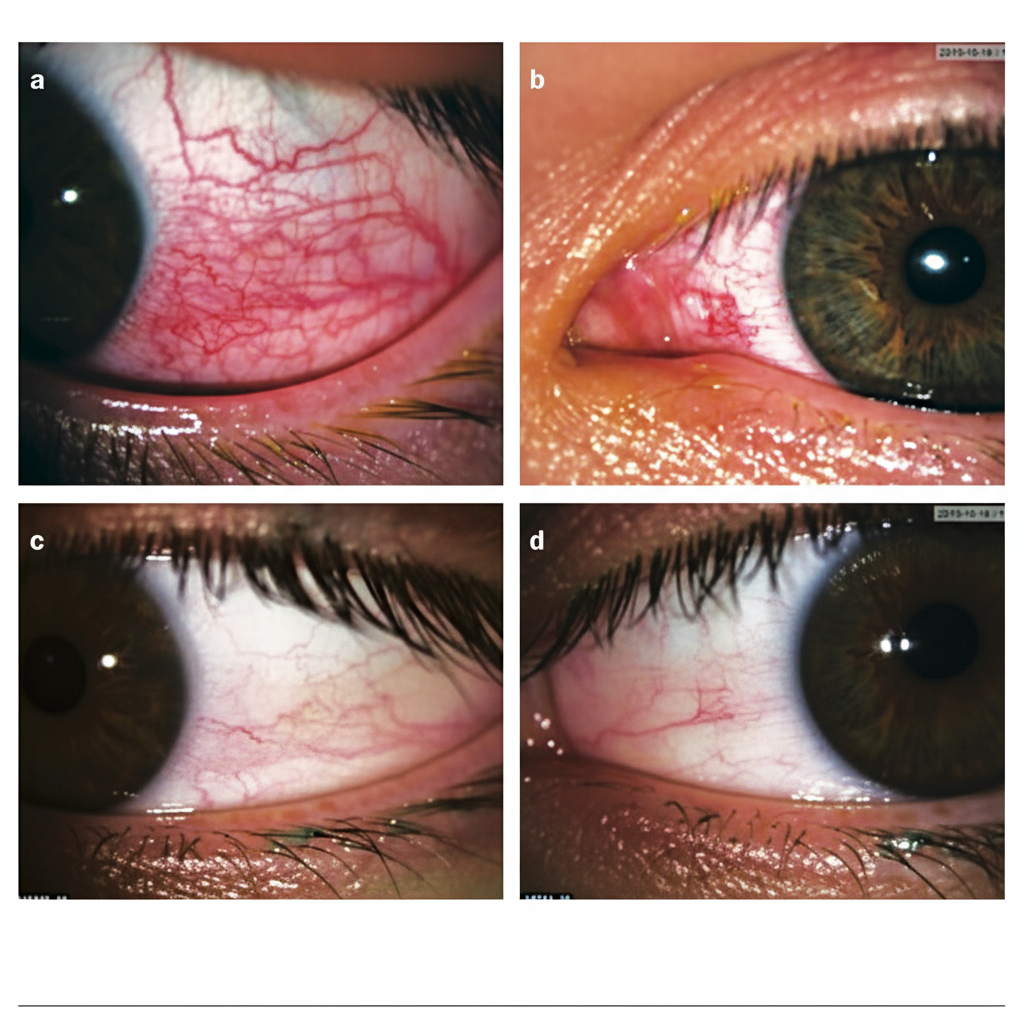
This image shows various degrees of conjunctival injection (redness) and engorged vessels, which are hallmark signs of conjunctivitis.
Now, let's talk about the itchy side of things: Allergic Conjunctivitis.
- Key Symptom: Itching is the absolute hallmark. If they aren't itching, it's probably not allergic!
- Vernal Keratoconjunctivitis (VKC): This is the "Spring Catarrh." It usually affects young boys and presents with cobblestone papillae on the upper tarsal conjunctiva and Trantas dots at the limbus.
- Atopic Keratoconjunctivitis (AKC): More chronic, associated with atopic dermatitis.
And then there's the Pterygium—that "wing-shaped" fold of conjunctiva that starts crawling onto the cornea.
- Etiology: It's heavily linked to UV exposure (think farmers or people living near the equator).
- Clinical Sign: Look for Stocker's line (iron deposition) at the leading edge.
- Management: If it's small, we just watch it. If it threatens the visual axis or causes significant astigmatism, we go for surgical excision with a conjunctival autograft (the gold standard to prevent recurrence).
Let me find some deep-dive lessons for you on these topics.
📚 Conjunctival Disease Lessons
Those lessons cover everything from the microbiology of Chlamydia (don't forget Trachoma!) to the specific types of conjunctivitis.
To help you lock in these differences—like the discharge types and the classic signs of VKC—let's pull up some flashcards.
🗂️ Conjunctival Disease Flashcards
Tap to study 18 flashcards in the Oncourse app
Those flashcards are great for testing your recall on the specific details, like the role of metalloproteinases in pterygium!
To wrap this up, here's a quick "cheat sheet" for your revision:
| Condition | Key Clinical Feature | Discharge Type | Management Highlight |
|---|---|---|---|
| Bacterial | Eyelids stuck in morning | Purulent (Yellow/Green) | Topical antibiotics (e.g., Moxifloxacin) |
| Viral | Preauricular nodes, Follicles | Watery/Serous | Supportive, cold compresses, hygiene |
| Allergic | Intense itching, Papillae | Mucoid/Ropy | Antihistamines, Mast cell stabilizers |
| Pterygium | Wing-shaped growth | N/A | UV protection; Surgery if vision threatened |
If you want to practice some clinical scenarios or see how these show up in exams, just let me know and we can pull up a quiz!
Setting up chat...