Common fractures: Colles, scaphoid, ankle — classification and management
Orthopedic trauma is a massive part of the UKMLA AKT, and these three fractures are the "bread and butter" of any A&E rotation. Let's break them down so you can spot them a mile away in your exam.
1. Colles Fracture
This is the classic "dinner fork" deformity. It's a distal radius fracture with dorsal displacement and angulation, usually from a Fall On an Outstretched Hand (FOOSH).
- Classification: Often described by the degree of comminution or intra-articular involvement (Frykman classification), but for the AKT, focus on the "dinner fork" description.
- Management:
- Undisplaced: Below-elbow backslab/cast.
- Displaced: Manual reduction (Hematoma block or Bier's block) followed by a cast.
- Unstable/Intra-articular: May require ORIF (Open Reduction Internal Fixation) with a volar plate.
Let me find a good visual of that classic deformity for you.
That X-ray on the right shows the classic dorsal displacement of the distal radius. Now, let's talk about the one that keeps orthopedic surgeons up at night because it's so easy to miss.
2. Scaphoid Fracture
Also from a FOOSH, but the pain is localized to the anatomical snuffbox. The big risk here is avascular necrosis (AVN) because the blood supply (the radial artery) enters from the distal end and flows proximally (retrograde).
- Classification (Herbert):
- Type A: Stable acute fractures.
- Type B: Unstable acute fractures (displaced or proximal pole).
- Management:
- Clinical suspicion but normal X-ray: Apply a scaphoid cast and re-image in 10-14 days (or go straight to MRI if available).
- Displaced or Proximal Pole: Often requires surgical fixation with a Herbert screw because the risk of non-union is so high.
I'll pull up a diagram showing that retrograde blood supply—it's the key to understanding why we worry about the proximal pole.
That diagram shows exactly why the proximal pole is so vulnerable—the fracture literally cuts off its only blood supply. Now, let's head down to the ankle.
3. Ankle Fractures
For the AKT, you need to know when to X-ray (Ottawa Ankle Rules) and how to classify them (Weber).
- Ottawa Ankle Rules: X-ray only if:
- Bony tenderness at the posterior edge or tip of the lateral or medial malleolus.
- Inability to bear weight both immediately and in the A&E (4 steps).
- Weber Classification:
- Weber A: Below the syndesmosis (usually stable).
- Weber B: At the level of the syndesmosis (may be unstable).
- Weber C: Above the syndesmosis (always unstable, requires ORIF).
- Management:
- Stable (Weber A): Weight-bearing boot or cast.
- Unstable (Weber C or some B): ORIF to restore the "mortise" (the joint's structural integrity).
Let's find a diagram of the Weber classification—it's the most high-yield visual for ankle trauma.
I've put together a quick comparison table and the key visuals for these three high-yield fractures. This should help you keep the classifications and management steps straight for your exam.
Common Fractures: Summary & Visuals
| Fracture | Mechanism | Key Classification | Management |
|---|---|---|---|
| Colles | FOOSH | Frykman (Intra-articular vs. Extra-articular) | Reduction + Cast (if displaced); ORIF (if unstable) |
| Scaphoid | FOOSH | Herbert (A-D) | Cast (even if X-ray normal); ORIF (proximal pole/displaced) |
| Ankle | Inversion/Eversion | Weber (A, B, C) | Weber A: Boot/Cast; Weber C: ORIF |
1. Colles Fracture (Dinner Fork Deformity)
 The right image shows the classic dorsal displacement and angulation of the distal radius.
The right image shows the classic dorsal displacement and angulation of the distal radius.
2. Scaphoid Blood Supply & AVN Risk
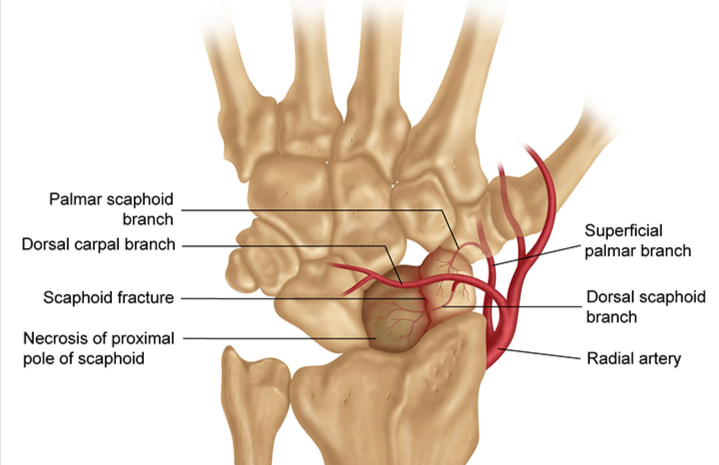 Note the retrograde blood supply—a fracture at the waist or proximal pole can easily lead to avascular necrosis.
Note the retrograde blood supply—a fracture at the waist or proximal pole can easily lead to avascular necrosis.
3. Weber Classification of Ankle Fractures
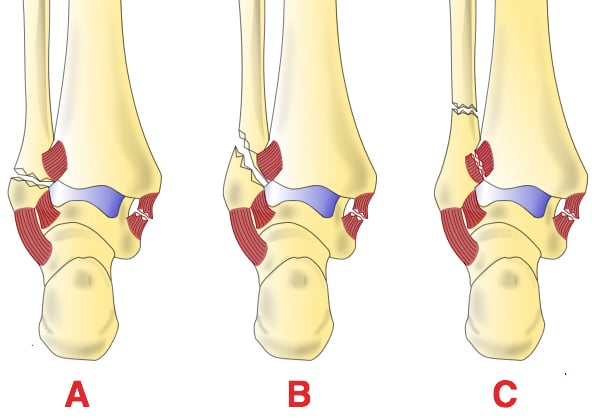 A: Below syndesmosis; B: At level of syndesmosis; C: Above syndesmosis (unstable).
A: Below syndesmosis; B: At level of syndesmosis; C: Above syndesmosis (unstable).
I've pulled up some key lessons that go into more detail on these fractures, especially the management algorithms which are super high-yield for the AKT.
📚 Fracture Management Lessons
To help you lock in those classification systems (especially Weber and Herbert), I've found some targeted flashcards for you to review.
🗂️ Fracture Revision Flashcards
Tap to study 7 flashcards in the Oncourse app
Those flashcards should help you nail the Ottawa rules—they're a classic AKT favorite!
If you want to test your knowledge on these, I can set up a quick quiz for you, or we could even run through a clinical case to see how you'd manage a patient in A&E. Just let me know!
Setting up chat...