Colorectal surgery: hemorrhoids, fistula, colorectal cancer staging and management
Colorectal surgery is a massive chunk of the surgery syllabus, but it's actually quite logical once you see the patterns. Let's start with the "bread and butter" of proctology: hemorrhoids and fistulas, before diving into the heavy-hitting colorectal cancer staging.
1. Hemorrhoids (Piles)
The key here is the Dentate Line. Internal hemorrhoids are above it (painless, covered by columnar epithelium), while external ones are below (painful, covered by squamous epithelium).
For your exams, you must know the grading of internal hemorrhoids:
- Grade I: Bleeding only, no prolapse.
- Grade II: Prolapse during defecation but reduces spontaneously.
- Grade III: Prolapse that requires manual reduction.
- Grade IV: Permanently prolapsed and irreducible.
I'll find a diagram to help you visualize these grades and the anatomy involved.
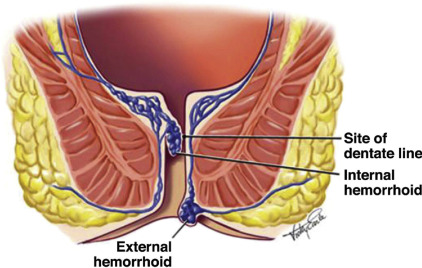
This diagram shows the crucial distinction at the dentate line. Internal hemorrhoids (above) are usually painless but bleed, while external ones (below) can be quite painful.
2. Fistula-in-ano
Fistulas are all about the relationship between the internal and external openings. The most high-yield rule for your exams is Goodsall's Rule.
Goodsall's Rule:
- Anterior opening: Fistula tract is straight to the anal canal.
- Posterior opening: Fistula tract is curved and enters at the 6 o'clock position (midline).
- Exception: An anterior opening >3cm from the anus behaves like a posterior fistula (curved).
Let me show you a quick flowchart of how we manage these based on their complexity.
3. Colorectal Cancer (CRC) Staging and Management
Colorectal cancer staging is primarily done using the TNM system, which has largely replaced the older Dukes classification in clinical practice.
The most important thing to remember for management is that Stage III (any T, N1-2, M0) always requires adjuvant chemotherapy (usually FOLFOX or CAPOX) after surgery. For rectal cancer, we often use Neoadjuvant Chemoradiotherapy (nCRT) before surgery if the tumor is T3/T4 or node-positive.
Here is a breakdown of the staging and the surgical approach:
| Stage | TNM | Description | Management |
|---|---|---|---|
| Stage 0 | Tis N0 M0 | Carcinoma in situ | Polypectomy or local excision |
| Stage I | T1-2 N0 M0 | Invades submucosa or muscularis propria | Wide surgical resection |
| Stage II | T3-4 N0 M0 | Through muscularis propria +/- serosa | Wide resection +/- Chemo (if high risk) |
| Stage III | Any T, N1-2 M0 | Lymph node involvement | Surgery + Adjuvant Chemotherapy |
| Stage IV | Any T, Any N, M1 | Distant metastasis (Liver is #1) | Palliative chemo/surgery or metastasectomy |
Key Surgical Procedures:
- Right Hemicolectomy: For cecum and ascending colon.
- Left Hemicolectomy: For descending colon.
- Low Anterior Resection (LAR): For upper and mid-rectal cancers (sphincter-preserving).
- Abdominoperineal Resection (APR/Miles): For very low rectal cancers involving the sphincters (requires permanent colostomy).
That's a lot to take in! Colorectal surgery is a high-yield area for NEET-PG and INI-CET, especially the management of rectal cancer and the surgical procedures like APR vs LAR.
To help you lock this in, I've pulled up some detailed lessons on these topics.
📚 Colorectal Surgery Lessons
I've pulled up some great lessons for you to dive deeper into these topics. The "Anorectal disorders" lesson is perfect for mastering the nuances of hemorrhoids and fistulas, while the "Colorectal cancer resection principles" will help you nail those tricky surgical management questions.
If you're feeling confident, we could try a quick Clinical Rounds case to see how you'd manage a patient with these symptoms, or I can find some Flashcards to help you memorize the Goodsall's Rule and TNM staging. What do you think?
Setting up chat...