Coeliac disease: serology, biopsy findings and gluten-free diet management
Coeliac disease is a classic UKMLA AKT topic because it’s so common and the management is very specific. It’s essentially an autoimmune-mediated sensitivity to gluten that leads to chronic inflammation of the small bowel.
I'll find some high-yield lessons to get us started on the specifics.
📚 Coeliac Disease Lessons
When we're looking at Coeliac disease, the diagnosis is a two-step process: serology first, then biopsy to confirm.
1. Serology: The First Step
The first-line test is IgA tissue transglutaminase (tTG). However, there's a major catch that examiners love: you must check the patient's total IgA levels at the same time.
Why? Because selective IgA deficiency is more common in people with Coeliac disease. If they don't produce IgA, their IgA tTG will be negative even if they have the disease! In those cases, we switch to checking IgG-based antibodies (like IgG tTG or IgG EMA).
AKT Tip: Patients must be on a gluten-containing diet for at least 6 weeks before testing. If they've already cut out gluten, the tests might come back falsely negative.
2. Biopsy: The Gold Standard
If the serology is positive, we move to a duodenal biopsy via an OGD (endoscopy). We usually take at least 4-6 samples because the damage can be patchy.
The classic "Marsh criteria" findings are:
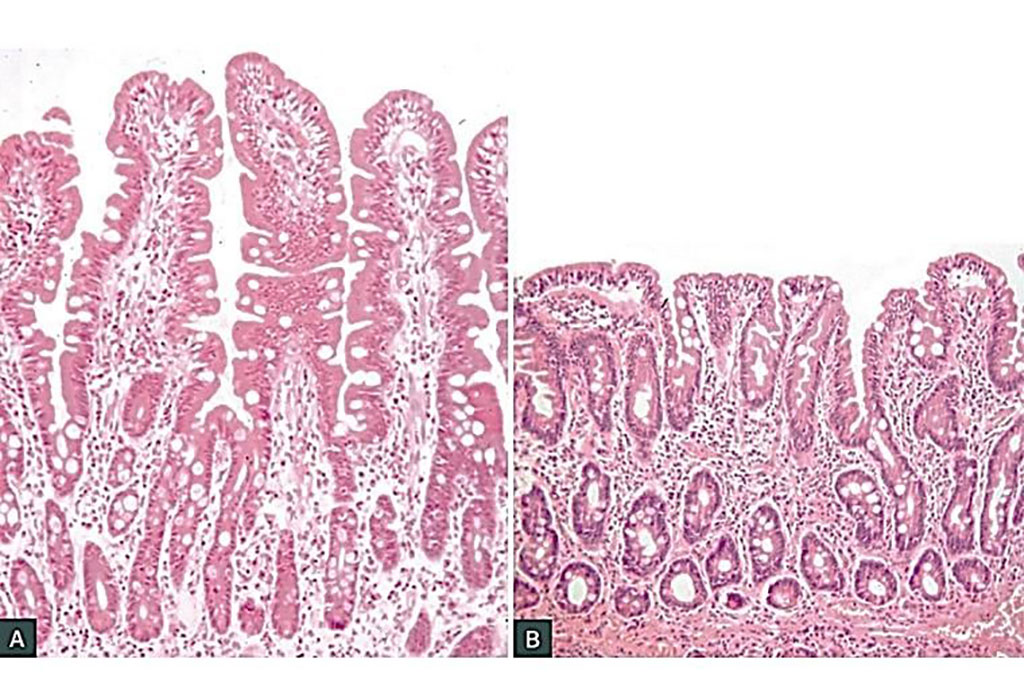
- Villous atrophy: The finger-like projections (villi) that absorb nutrients get flattened.
- Crypt hyperplasia: The "valleys" between the villi get deeper as the body tries to regenerate cells.
- Increased intraepithelial lymphocytes (IELs): Lots of white blood cells moving into the lining.
Let me find a diagram or image of this histology so you can see the difference between healthy and coeliac tissue.
Here is a side-by-side comparison of normal intestinal villi versus the flattened villi seen in Coeliac disease.
3. Management: Beyond Just "No Bread"
The management of Coeliac disease is lifelong and involves more than just dietary changes. Here’s the high-yield breakdown for your exams:
| Aspect | Management Detail |
|---|---|
| Diet | Lifelong Gluten-Free Diet (GFD). This means no wheat, barley, or rye. Oats are often okay but can be contaminated. |
| Referral | All patients should be referred to a specialist dietitian for education on hidden gluten (like in sauces or beer). |
| Vaccination | Pneumococcal vaccine (and sometimes others) is required because Coeliac disease causes functional hyposplenism. |
| Bone Health | Malabsorption of Vitamin D and Calcium increases the risk of osteoporosis. A DEXA scan is often recommended at diagnosis. |
| Monitoring | Annual review to check symptoms, weight, and sometimes repeat serology to monitor adherence to the diet. |
| Feature | Coeliac Disease Summary |
|---|---|
| First-line Test | IgA tTG (Check total IgA!) |
| Gold Standard | Duodenal Biopsy (Villous atrophy, Crypt hyperplasia) |
| Dietary Trigger | Gluten (Wheat, Barley, Rye) |
| Key Complication | Functional Hyposplenism (Needs Pneumococcal vaccine) |
| Long-term Risk | Osteoporosis, Small bowel lymphoma (rare) |
That summary table covers the most frequent ways Coeliac disease shows up in the AKT.
One last thing to remember: if a patient is diagnosed with Coeliac disease, it's also recommended to screen their first-degree relatives (parents, siblings, children) because there's a strong genetic component (HLA-DQ2 and HLA-DQ8).
If you're feeling confident about the theory, we could try a quick quiz or even a clinical case to see how this looks in practice!
Setting up chat...