Chronic kidney disease: staging, complications and when to refer to nephrology
Chronic Kidney Disease (CKD) is a massive topic for the UKMLA AKT, and it's essentially defined as a reduction in kidney function (eGFR < 60) or evidence of kidney damage (like albuminuria) for at least 3 months.
The staging system is the "bread and butter" here—it's a dual system using both eGFR (G stage) and Albumin:Creatinine Ratio (ACR, A stage). This is crucial because a high ACR significantly increases cardiovascular risk and the rate of progression, even if the eGFR is relatively stable.
I've put together the standard NICE staging table for you to help visualize how these two metrics interact.
| G stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Normal or high |
| G2 | 60–89 | Mildly decreased |
| G3a | 45–59 | Mildly to moderately decreased |
| G3b | 30–44 | Moderately to severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | < 15 | Kidney failure |
| A stage | ACR (mg/mmol) | Description |
|---|---|---|
| A1 | < 3 | Normal to mildly increased |
| A2 | 3–30 | Moderately increased |
| A3 | > 30 | Severely increased |
When the kidneys start to fail, they stop doing their "side jobs," which leads to a cascade of complications. The most common cause of death in CKD patients isn't actually kidney failure—it's Cardiovascular Disease (CVD), so managing blood pressure and lipids is priority number one.
Other high-yield complications include:
- Anemia: Usually normocytic/normochromic due to reduced Erythropoietin (EPO) production.
- CKD-Mineral Bone Disorder (MBD): A complex dance of low Vitamin D, low Calcium, and high Phosphate, leading to Secondary Hyperparathyroidism.
- Electrolyte disturbances: Particularly Hyperkalemia and metabolic acidosis as the kidneys lose their ability to excrete acid and potassium.
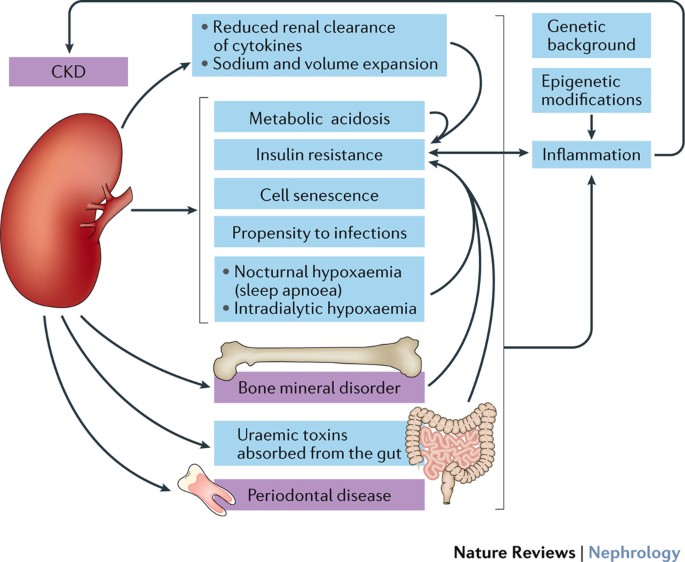
Let me find a visual that summarizes these systemic effects for you.
This diagram gives a great overview of how CKD isn't just a kidney problem—it's a systemic inflammatory state that affects everything from your bones to your heart.
Finally, knowing when to refer to a nephrologist is a common AKT question. Generally, you're looking for signs of rapid progression, severe damage, or complications that are hard to manage in primary care.
According to NICE, you should refer if:
- eGFR < 30 (Stage G4 or G5).
- ACR ≥ 70 (unless due to diabetes and already appropriately treated).
- ACR ≥ 30 PLUS hematuria.
- Rapid decline in eGFR (defined as >5 mL/min in 1 year, or >10 mL/min in 5 years).
- Resistant hypertension (not controlled on 4 or more drugs).
- Suspected rare or genetic causes (like Polycystic Kidney Disease).
I've summarized these referral triggers in a quick-reference table for you.
| Referral Criterion | Details |
|---|---|
| eGFR Threshold | eGFR < 30 mL/min/1.73 m² (G4/G5) |
| Albuminuria (ACR) | ACR ≥ 70 mg/mmol (unless diabetic and treated) |
| ACR + Hematuria | ACR ≥ 30 mg/mmol with persistent microhematuria |
| Rapid Progression | eGFR drop > 5 in 1 year or > 10 in 5 years |
| Hypertension | Poorly controlled BP despite ≥ 4 antihypertensives |
| Specific Causes | Suspected renal artery stenosis or genetic disease (e.g., ADPKD) |
To help you lock this in for your exam, I've pulled some key lessons and flashcards on CKD management and complications.
📚 CKD Lessons for AKT
And here are some flashcards to test your recall on these criteria and complications.
🗂️ CKD Flashcards for AKT
Tap to study 6 flashcards in the Oncourse app
CKD is all about managing the long-term risks, especially cardiovascular health. If you can keep the blood pressure under control and catch those complications like anemia and bone disease early, you're doing a great job for your patients.
Good luck with your AKT prep—you've got this!
Setting up chat...