Childhood asthma: BTS/SIGN stepwise management and inhaler technique
Hey! Childhood asthma is a massive topic for the UKMLA AKT. The BTS/SIGN guidelines are the bread and butter of pediatric respiratory questions, so let's get you comfortable with the steps.
The management is split by age groups because little lungs need different approaches. I've put together a summary table of the BTS/SIGN stepwise approach for you to keep these straight.
| Step | Children < 5 Years | Children 5-12 Years |
|---|---|---|
| Step 1 | SABA prn (e.g., Salbutamol) | SABA prn (e.g., Salbutamol) |
| Step 2 | Low-dose ICS (if symptoms >3x/week or night waking) | Low-dose ICS |
| Step 3 | Add LTRA (e.g., Montelukast) | Add LABA (e.g., Salmeterol) - Stop LABA if no response |
| Step 4 | Refer to Specialist | Increase ICS dose OR Add LTRA |
| Step 5 | - | Refer to Specialist |
Key High-Yield Facts:
- ==Always check compliance and inhaler technique before moving up a step.==
- For children <5, if LTRA doesn't work at Step 3, you refer them.
- For children >5, if the LABA provides some benefit but not enough, you keep it and increase the ICS. If it does nothing, you scrap it.
Now, even the best meds won't work if they don't reach the lungs. For kids, the technique is everything.
Metered Dose Inhalers (MDI) with a Spacer are the gold standard for children. It reduces the need for coordination and ensures more drug reaches the small airways. For very young children (usually <3 years), a face mask is added to the spacer.
Here's a quick breakdown of the technique:
- Shake the inhaler and remove the cap.
- Attach the inhaler to the spacer.
- Seal the mask over the nose and mouth (or use the mouthpiece).
- Press the inhaler once.
- Breathe normally for 5-10 breaths (tidal breathing) or take one deep breath and hold for 10 seconds.
- Wait 30-60 seconds before the next puff.
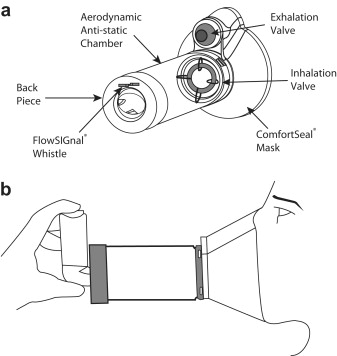
I'll find a diagram to help you visualize the spacer setup.
This diagram shows exactly how the spacer (valved holding chamber) works with the MDI. Notice the mask for younger kids and the one-way valve that lets them take multiple breaths to clear the chamber.
That's the core of it! To help you lock this in for the UKMLA, I've pulled up some high-yield lessons on childhood asthma and respiratory management.
📚 Childhood Asthma Lessons
Those lessons should give you a solid foundation for the AKT.
Since the BTS/SIGN steps can be a bit of a memory maze, would you like to try a quick game to see if you can group the right treatments with the right age groups and steps? It's a great way to make sure those guidelines stick!
Setting up chat...