Chest radiology: X-ray interpretation, common patterns and CT findings
Chest radiology is the bread and butter of clinical practice, especially for those high-yield exam questions! Whether you're looking at a standard PA view or a detailed HRCT, having a systematic approach is the only way to make sure you don't miss those subtle findings.
Let's start with a solid foundation for interpreting a Chest X-ray (CXR). I'll pull up a visual guide to help us walk through the systematic approach.
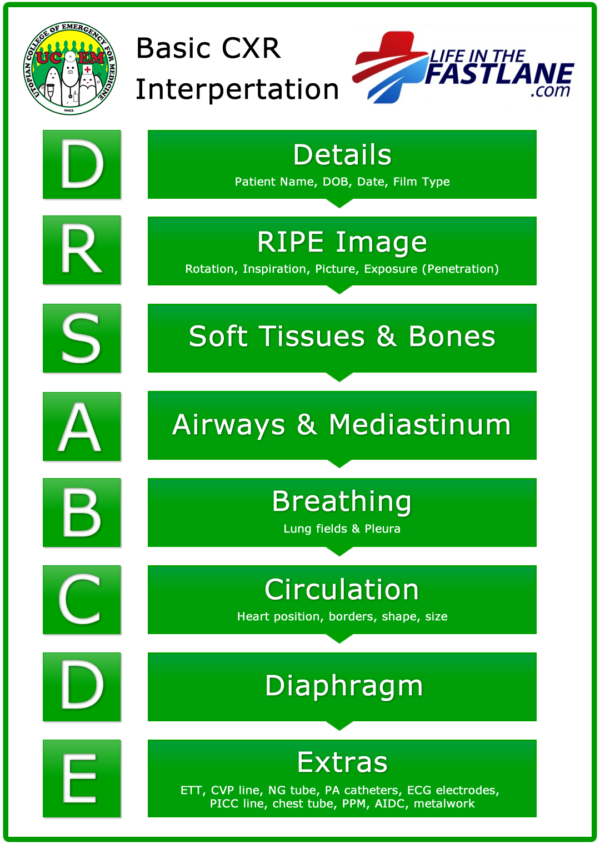
This guide covers the essential steps: from checking patient details and technical quality (RIPE) to systematically evaluating the airway, breathing, circulation, diaphragm, and extras.
When you're looking at the lung fields, you're essentially looking for "white" where there should be "black" (opacities) or "blacker" where there should be "black" (hyperlucency). Here's a quick breakdown of the most common patterns you'll encounter in your exams and on the wards.
| Finding | CXR Characteristics | Common Causes |
|---|---|---|
| Consolidation | Homogeneous opacity, Air bronchograms, Silhouette sign | Pneumonia, Pulmonary edema, Hemorrhage |
| Pleural Effusion | Blunting of costophrenic angles, Meniscus sign, Mediastinal shift (if large) | CHF, Malignancy, Infection (Parapneumonic) |
| Pneumothorax | Visible visceral pleural line, Absence of lung markings peripherally | Trauma, Spontaneous (Primary/Secondary), Iatrogenic |
| Collapse (Atelectasis) | Opacity with volume loss (displaced fissures, elevated diaphragm) | Mucus plug, Foreign body, Bronchial tumor |
| Nodules/Masses | Discrete opacities (<3cm = nodule, >3cm = mass) | Malignancy, Granuloma, Abscess |
| Pulmonary Edema | Kerley B lines, Bat-wing opacities, Cephalization of vessels | Left heart failure, Fluid overload |
When an X-ray isn't enough, we turn to High-Resolution CT (HRCT), which is the gold standard for interstitial lung diseases (ILD) and bronchiectasis. Here are the "big three" patterns you'll see in CT reports:
- Ground-Glass Opacity (GGO): Hazy opacification that doesn't obscure the underlying vessels. It usually indicates active, potentially reversible inflammation (like in early ILD or COVID-19).
- Honeycombing: Clustered cystic airspaces (usually 3-10mm) with thick walls, typically seen in the subpleural regions. This is a sign of irreversible fibrosis, classic for Usual Interstitial Pneumonia (UIP).
- Tree-in-Bud Pattern: Small, branching centrilobular nodules that look like a budding tree. This is a classic sign of small airway inflammation, often seen in infections like TB or bronchopneumonia.
To help you master these concepts for your exams, let me pull up some high-yield lessons on chest radiology and HRCT patterns.
📚 Chest Radiology Lessons
I've pulled up some great lessons that cover everything from normal anatomy to complex interstitial lung disease patterns. These are perfect for your revision!
Chest radiology is all about pattern recognition. The more you see, the better you get. For your exams, keep an eye out for those "buzzwords" like Silhouette sign (loss of a border between two structures of similar density) or Air bronchograms (air-filled bronchi seen against opaque lung).
Would you like to test your knowledge of these radiology patterns with a quick game? I can set up a Synapses game to help you group these findings with their most likely diagnoses!
Setting up chat...