CCS case: ordering diagnostic tests efficiently
Ah, the USMLE Step 3 CCS cases! That's where the real "doctoring" happens, and efficiency is the name of the game. It's not just about getting the right diagnosis; it's about how you get there without wasting time or resources.
Think of diagnostic testing in CCS like a funnel: you start with the broad, non-invasive "emergency" stuff and then narrow it down as the patient stabilizes.
The "Initial Orders" Rule of Thumb
For almost every patient who isn't 100% stable, you should have a "reflex" set of orders you place immediately. These are your "bread and butter" tests that give you a baseline without delaying care.
- Pulse Oximetry & Oxygen (if needed)
- IV Access & Normal Saline (if unstable)
- Cardiac Monitor & EKG (for any chest pain, SOB, or syncope)
- Basic Labs: CBC, BMP (or Chem-7), LFTs, and UA.
Efficient Ordering Strategy
To keep your efficiency score high, follow this logical progression:
- The "STAT" Phase: If they're unstable, fix the ABCs first. Don't order a CT scan for a patient with a tension pneumothorax; needle decompress first!
- The "Screening" Phase: Order your non-invasive tests together. If you suspect a PE, order the EKG, Chest X-ray, and ABG at the same time.
- The "Confirmatory" Phase: Only move to invasive or expensive tests (like a biopsy or CT with contrast) once the basics point you in that direction.
- The "Monitoring" Phase: Don't forget to re-order labs if the patient's condition changes or if you're managing something like DKA (where you need frequent BMPs).
I've got a great flowchart that breaks down the clinical decision-making process for efficient ordering. Let me pull that up for you!
This flowchart illustrates how you should think about sequential testing. In CCS, you often start with a highly sensitive "Assay 1" (like a screening lab) and only move to more specific "Assay 2" or "Assay 3" tests if the initial results warrant it.
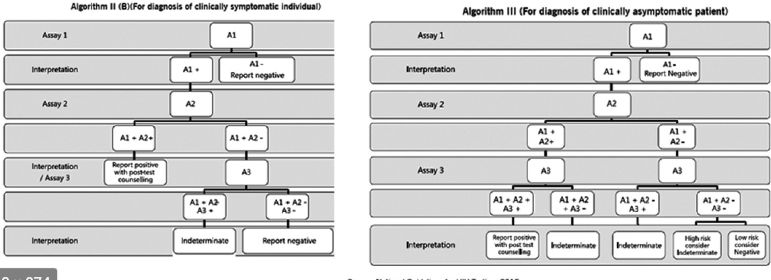
This algorithm demonstrates the importance of sequential testing—starting with a screening test and moving to confirmatory tests based on the initial results to ensure diagnostic accuracy and efficiency.
Pro-Tips for the CCS Interface:
- Physical Exam First: Always do a focused physical exam before ordering labs unless the patient is literally dying. It's "free" time-wise and gives you clues.
- Advance the Clock: After ordering, don't just sit there. Advance the clock to "Results of next available lab" to see what you've got.
- Cancel Unnecessary Tests: If you ordered something by mistake or the diagnosis becomes clear before the test is done, cancel it! It shows you're thinking about cost-effectiveness.
Would you like to try a practice case to see how this works in action, or should I find some high-yield lessons on common CCS scenarios?
Setting up chat...