Cardiac arrhythmias: identification, classification and treatment
Oh, cardiac arrhythmias! This is one of those topics that can feel like a tangled mess of wires at first, but once you get the rhythm down, it's actually quite logical. Think of the heart like a house where the electrical wiring has gone a bit rogue—sometimes it's too slow, sometimes it's too fast, and sometimes it's just plain chaotic.
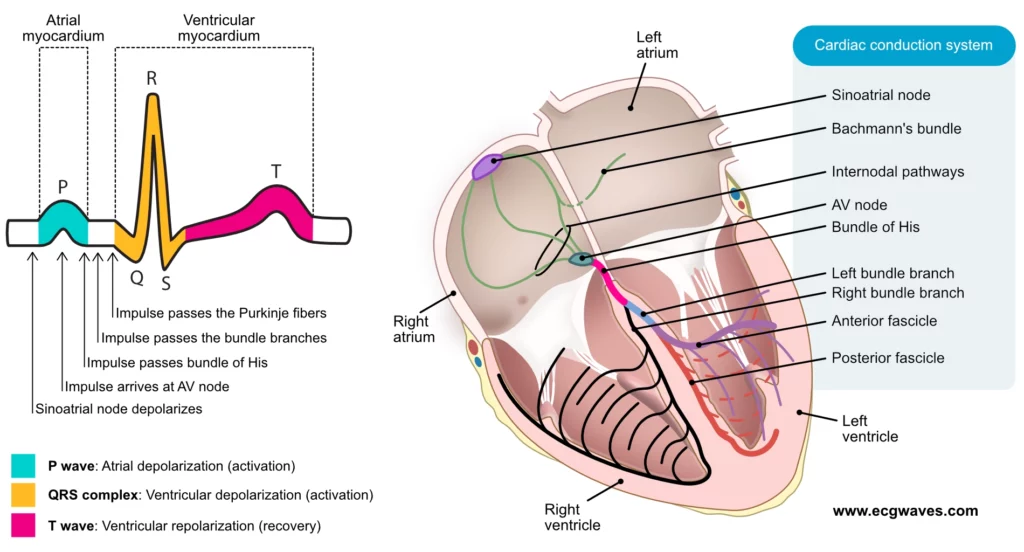
To get us started, let's look at the basic electrical conduction system of the heart, which is where all these rhythms begin (or go wrong).
This diagram shows how the electrical signal normally travels from the SA node down to the Purkinje fibers. When this path is interrupted or a new "spark" starts somewhere else, we get an arrhythmia.
Broadly speaking, we classify arrhythmias based on their rate (too fast or too slow) and their origin (above or below the ventricles).
1. Classification Overview
| Category | Heart Rate | Common Examples |
|---|---|---|
| Bradyarrhythmias | < 60 bpm | Sinus Bradycardia, AV Blocks (1st, 2nd, 3rd degree) |
| Tachyarrhythmias | > 100 bpm | SVT, Atrial Fibrillation, Ventricular Tachycardia |
Within Tachyarrhythmias, we look at the QRS complex width:
- Narrow QRS (< 120ms): Originates above the ventricles (Supraventricular).
- Wide QRS (> 120ms): Originates in the ventricles (Ventricular) or has aberrant conduction.
2. Identification (The ECG Clues)
When you're looking at an ECG, ask yourself these three questions:
- Is it regular or irregular? (Check the R-R intervals)
- Are there P waves? (If not, think Atrial Fibrillation or Junctional rhythms)
- Is the QRS narrow or wide?
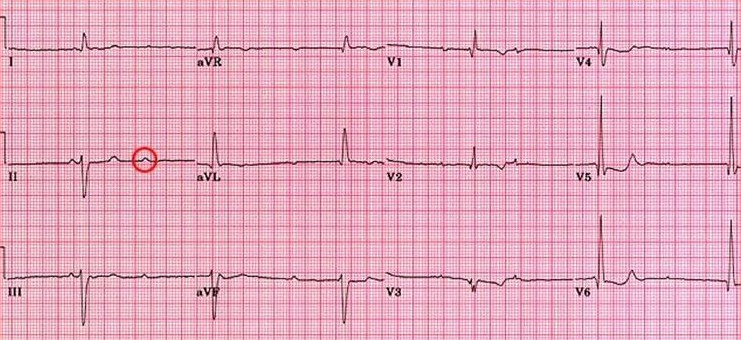
Let's look at one of the most common "irregularly irregular" rhythms you'll see on exams and in the clinic: Atrial Fibrillation (AFib).
This ECG shows the classic "irregularly irregular" rhythm of AFib. Notice the lack of clear P waves and the varying R-R intervals.
When it comes to treatment, the first question is always: Is the patient stable or unstable?
3. Treatment Principles
If the patient is unstable (hypotension, altered mental status, chest pain, or signs of shock), the answer is usually immediate action:
- Bradycardia: Atropine or Pacing.
- Tachycardia: Synchronized Cardioversion (if there's a pulse) or Defibrillation (if there's no pulse, like in V-Fib).
For stable patients, we can use medications:
| Arrhythmia | Common Treatment |
|---|---|
| Atrial Fibrillation | Rate control (Beta-blockers, CCBs) or Rhythm control (Amiodarone, Flecainide) + Anticoagulation (CHADS-VASc score). |
| SVT (AVNRT) | Vagal maneuvers, then Adenosine (6mg, then 12mg). |
| Ventricular Tachycardia | Amiodarone or Procainamide (if stable). |
| Bradycardia (Sinus) | Atropine (if symptomatic). |
Mnemonic: ABCD for AFib Anticoagulation, Beta-blockers, Cardioversion, Digoxin (less common now).
I've got some great lessons and flashcards that dive deeper into each of these rhythms. Let me pull those up for you!
📚 Arrhythmia Lessons
Those lessons are a great place to start, especially the one on common arrhythmia recognition. To really lock this in, let's look at some flashcards for quick review.
🗂️ Arrhythmia Flashcards
Tap to study 18 flashcards in the Oncourse app
Those flashcards are perfect for testing your recall on the fly. Since we've covered a lot of ground—from identification to management—how about we put your skills to the test with a quick game? It's a great way to see if you can distinguish between these rhythms under pressure!
Setting up chat...